

Immunization rates among Peel students have plummeted since the pandemic
Last month, Hamilton Public Health reported a child under the age of five had died after contracting the measles, marking the first death from the preventable virus identified via provincial monitoring since 1989. It was later reported the child was unvaccinated.
It is a growing trend emerging across the province and particularly in Peel.
A Public Health Ontario report from July 2023 revealed the number of seven-year-olds considered to be fully vaccinated against measles dropped from 78 percent in 2019-2020 to 39 percent in 2021-2022. In Peel the number fell to 37 percent.
Measles is only one of the nine designated diseases for which a vaccination record is required for school aged children in Ontario — unless a valid exemption is accepted. The others include Diphtheria, Tetanus, Polio, Meningococcal, Pertussis (whooping cough) and Varicella (chickenpox).
A recent report from Public Health Ontario, which oversees 34 local Public Health Units, revealed 22 cases of the measles in Ontario so far this year, the same number in the twelve months of 2014, which was a recent record high. Thirteen of this year's cases have occurred in children and in twelve of those cases the child was not immunized — the immunization status of the thirteenth child is unknown.
Measles, a viral respiratory tract infection causing a high fever, cough, runny nose and full body rash, is most common in children but can infect people at any stage of life. In 1998 measles was declared to be eliminated from Canada due to the success of vaccination programs. The MMR vaccine — which protects against measles, mumps and rubella — is administered to children first between the ages of 12 to 15 months, and again at 18 months, which is considered a life-long protection with a vaccine efficacy of over 90 percent.
But in recent years measles has been making a comeback, largely attributed to increased movement of people, denial of the benefits of immunization and vaccine complacency.
Most measles cases in Canada have reportedly been contracted during travel overseas. Currently Europe is struggling with one of the largest measles outbreaks in decades with over 30,000 cases reported in 2023. Cases escalated near the end of last year and continued into 2024. India, where a large percentage of Peel’s population traces their roots to, recently had the fourth highest reported number of total measles cases, according to the World Health Organization (WHO).
International travel was limited as a result of the COVID-19 pandemic, but numbers have quickly rebounded to pre-pandemic levels — in 2023, approximately 45 million people travelled through Pearson International Airport, close to the 50.5 million seen in 2019. The airport authority says there is an estimated ten percent day to day increase in passengers moving through Pearson this year compared to 2023.
With Peel’s large immigrant population continuing to grow rapidly, as some 200,000 residents move here by 2031, different immunization policies in other countries pose a challenge to local public health officials.
“With this growth we are seeing people who are vulnerable to infectious diseases, including newcomers to Canada, like myself a few years ago, and visitors from countries with higher rates of some communicable diseases and different immunization schedules than Toronto's or Ontario's,” Nazia Peer, Director of Immunization Services at the Region of Peel, told Regional Council recently.
The Region saw its first confirmed case of measles this year on February 13, when an unvaccinated one-year-old tested positive following international travel. The infant had multiple exposure locations which prompted an urgent response from the Public Health Unit to identify anyone that might have been exposed.
“We also receive many calls from an anxious public. This one confirmed case generated 380 contacts,” Judy Buchan, Director of Communicable Diseases and Chief Nursing Officer, told councillors. “Each contact received either a text, a letter and/or a phone call based on their risk to provide education and our instructions for exclusion from high risk settings. Every one of those 380 contacts has a story of how they were affected by this exposure.”
Due to the extremely high contagiousness of measles, Ontario Public Health aims for a minimum 95 percent vaccination coverage rate to protect communities against the transmission of the virus. In recent years, the rate of vaccination against MMR in particular has sharply declined.

Routine childhood immunizations are one of the most important public health measures to limit the spread of communicable diseases.
(CDC)
MMR is also not the only vaccine being ignored by an increasing number of Ontarians. Buchan, told Peel Council that 50 percent of students across the Region’s four publicly funded school boards were missing a record of at least one dose of a vaccine required to attend school. Across the Region there are 421 schools and 227,780 students registered across Peel’s three municipalities with Peel District School Board being the largest. More than 100,000 students are missing a record of at least one dose of one required vaccine.
According to the Canadian Public Health Association, immunization has saved more lives and reduced the spread of infectious diseases more than any public health measure over the past 50 years. Recognizing the importance of the fairly simple measure, Peel Public Health is looking to Council for support in its efforts to increase the service capacity to deal with the catch up of immunization records that have been greatly hindered by the COVID-19 pandemic.
On Thursday, Council approved the addition of ten contract positions in Public Health from July 1, 2024 to March 31, 2026 at a cost of $1.2 million, and the extension of 37 existing contract positions and eight existing student positions until March 31, 2026 at a cost of $7.3 million, using funds from the COVID-19 Recovery Reserve.
During the pandemic, routine immunization services were limited, playing a role in the downward trend of fully vaccinated children. At the height of the pandemic, deployment of public health services and primary care services were limited which precludes vaccinations. In addition, school closures removed one of the most easily accessible vaccine measures for families. Peel schools have implemented programs that administer immunization for Hepatitis B, Meningococcal, and Human Papillomavirus (HPV), which became unavailable during school closures. As a result, routine school immunization coverage rates for these three communicable diseases are 10 to 36 percent below pre pandemic benchmarks.
“Although most of the world has moved on since the pandemic, the public health world is experiencing a post pandemic reality of increasing communicable diseases at a global level,” Peer said. “We are seeing the resurgence of vaccine preventable diseases like measles, mumps, diphtheria, and cholera, and the emergence of other communicable diseases like M pox, which pose risks to our community, especially those who are most vulnerable. And Peel is not immune from what is happening across the world, because these global infectious diseases, or the trends directly impact the Peel community.”
Peel Public Health is mandated by the Health Protection and Promotion Act (HPPA) and the Ontario Public Health Standards to provide case and contact management of more than 25 Diseases of Public Health Significance including measles, influenza and invasive Group A Streptococcal disease (commonly known as strep throat) among others.
According to Peel Public Health’s annual review for 2023, the Region saw a 30 percent increase in respiratory tuberculosis, 91 percent increase in invasive Group A Streptococcus, 154 percent increase in HIV, 40 percent increase in infectious syphilis and 17 percent increase in gonorrhea compared to 2018 to 2022.
As Public Health grapples with chronic resource constraints, there are increasing instances of outbreaks, demanding greater control across the Region. Those living in congregate settings, including retirement homes, long term care facilities, group homes, temporary shelters and others, are at greater risk for contracting and spreading disease due to shared living spaces.

Those living in congregate settings, such as long term care homes, are at greater risk for contracting communicable diseases.
(Danie Franco/Unsplash)
One of the two staff reports presented to Regional Council Thursday determined that outbreaks in congregate living settings remain higher than pre pandemic years. Institutional outbreaks of communicable diseases — an outbreak is defined as two or more cases linked to each other — were 6.6 times higher in 2023 compared to the pre pandemic average (2015-2019).
During the pandemic, public health resources were also largely diverted. Peel quickly became one of the biggest COVID-19 hotspots in Ontario, fueled by racism, intergenerational living, crowded long term care homes and insufficient hospital space, leading to the management of over 200,000 confirmed and probable cases and over 1,700 outbreaks. By April 2021, Brampton had a COVID test positivity rate almost double that of the province.
When the first COVID vaccine became publicly available in the first half of 2021, Peel residents flocked to temporary public health clinics for their jab. By May 2022, over 3,350,000 doses of a coronavirus vaccine had been administered across the Region with 90.4 percent of the eligible population (age five and above) having received at least one dose and 87.2 percent were fully vaccinated.
But as pop up clinics were filled to the brim with masked residents, and all public health resources were diverted to the crisis, the COVID-19 vaccine took precedence over other immunizations, creating a backlog that the public health body is now looking to catch up on.
As outbreaks persist, Peel Public Health’s capacity is being challenged, begging the need for continued investment and support.
“[It is] putting the health and safety of Peel residents at significant risk. Our resource limitations both in communicable disease and the immunization services divisions are really stretched in terms of responding optimally,” Peer said. “Without an urgent investment in resources to match the population growth and the global disease trends, Peel’s public health services will continue to fall below the mandated standards and legislative requirements.”
Peel Public Health has not shied away from publicizing the lack of financial support it receives from the Ontario government, and it is not an issue that has arisen recently. For over a decade, Ontario’s fastest growing region has repeatedly received scrapings from the bottom of the barrel.
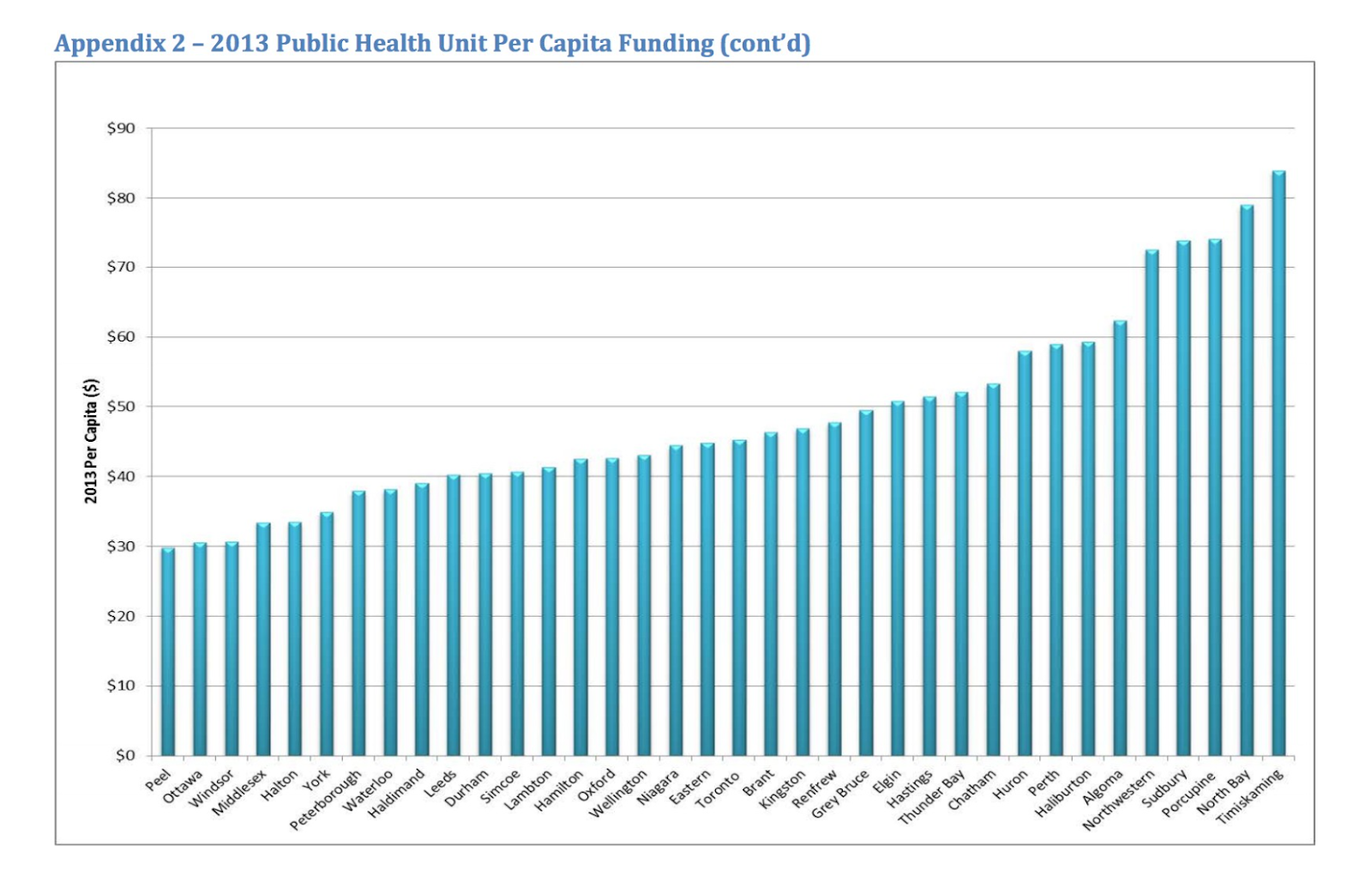
Peel Public Health has repeatedly received less funding than its counterparts in other Ontario regions.
(Government of Ontario)
In 2013, a per capita review of all Public Health units across Ontario was completed. Peel ranked last for provincial funding, receiving only $29.83 per capita — compared to the highest receiving unit in Timisking which received almost $85 per capita. But the decade old study is only a snapshot of a funding problem that has followed a roller coaster path for the better part of three decades.
In the early 90s, Ontario maintained a 75/25 funding split, between the provincial and municipal governments, for mandatory public health programming including controlling infectious and chronic diseases, environmental health, injury prevention and family health. Under former PC premier Mike Harris, who held provincial office from 1995 to 2002, funding for public health units became the sole responsibility of municipalities. In 1998, zero percent of funding came from the province. In 1999, the funding model shifted back to 50/50.
The goal was to return to a 75/25 split in three years, an ambition that was unsuccessful when funding was capped in 2011 with only 17 Public Health units reaching this funding level split. Currently the target split is 70/30. Peel never rebounded to this level, and in 2023, the Region’s Public Health unit was only funded 51 percent by the province, with the remaining 49 percent coming from the municipalities. The lack of substantial financial support from the province has left the sector with a $9.9 million funding shortfall in its 2023 budget, increasing from an $8.1 million shortfall in 2022 when the funding split was 61/39. Funding has been frozen since 2018, with the exception of a minor increase in 2019.
“It has been quite some time since this health unit was at the 70/30 split intended by the HPPA (Health Protection and Promotion Act). And we are farther off the 60/40 split that we were at pre-pandemic,” Buchan said, stating she would be returning back to Council in June to present the public health funding situation. “It certainly hasn't gotten any better in the intervening years. And we also have a number of years where we haven't been before council to ask for any permanent resources because of the pandemic. So we really have four or five years of disruption that will require a catch up in the meantime.”
The Region of Peel’s 2024 Capital Budget allocates $350,000 for Public Health projects with a carry forward of $7 million for existing projects. The operating budget increased slightly from $37.8 million in 2023 to $40.1 million in 2024, which includes an additional seven full time employment contracts. But programming and staffing has become increasingly unstable in the competitive job market with 40 percent of staff in temporary contract positions.
Council’s approval of the use of funds from the COVID-19 Recovery Reserve is money that formed as a surplus during the peak years of the pandemic. When nurses and other public health professionals were redirected from their usual posts to aid in the emergency pandemic response, the provincial government paid for this work, running a surplus in Peel of approximately $41 million. This is now money that the Public Health Unit can use to catch up on measures that were sidetracked during the pandemic.
As Public Health continues to deal with the backlog, the only challenge they face is not the growing number of people requiring immunizations, but also the changing social dynamics around Public Health measures in general. While Public Health Ontario has widely publicized the effectiveness of vaccines, as was evident through the COVID-19 pandemic, continual pressures to receive one, two, three and even four doses of the COVID-19 vaccine have begun to cause what some are calling “vaccine fatigue”.
The phenomenon is described by the American National Institutes of Health as an “inertia or inaction towards vaccine information or instruction due to perceived burden or burnout”. This was seen throughout the later years of the pandemic as less of the population showed up to receive booster doses of the COVID-19 vaccine for various reasons including mixed messaging, avoidance of side effects, and frequency of vaccination demands.
This circumstance is symbolic of the human side of Public Health workers’ jobs. The solution to the growing backlog of routine vaccinations cannot be solved as simply as making the vaccines more widely available. Public Health must also continue to educate the public on the importance of these routine vaccinations and the dangers of the spread of communicable diseases.
“Many measles contacts include parents of children who are already sick, dealing with a medical condition that sent them to either the health clinic or the emergency department in the first place,” Buchan said. “But then they must also cope with being informed by our nurses that they are now contacts of a highly infectious communicable disease. Counseling stressed parents is an important part of our job.”
Buchan described one situation during the February 13 confirmed measles case of a woman who was excluded from her workplace after being unable to prove she was immunized for measles and, in turn, faced financial hardship. When no record of immunization could be found, a nurse performed a blood test.
“The nurse continued to provide emotional support during this process, helping her to manage the stress that the situation put her under. Fortunately, we were able to confirm her immunity through a blood test when the results came in, and the contact was quickly able to return to work,” Buchan said. “She certainly appreciated all the support she received from public health and the nurses involved. Measles cases are time consuming. They are expensive to manage and they take staff away from other important work. This story however, really illustrates the human impact, the health impact and the financial impact on our residents when they are exposed to a case.”
Buchan said her team will be returning to council later in the year to advocate for funding in the 2025 budget, but for the time being is urging both council and the public to not only look at the numbers, but the people behind them.
Email: [email protected]
Twitter: @rachelnadia_
At a time when vital public information is needed by everyone, The Pointer has taken down our paywall on all stories to ensure every resident of Brampton, Mississauga and Niagara has access to the facts. For those who are able, we encourage you to consider a subscription. This will help us report on important public interest issues the community needs to know about now more than ever. You can register for a 30-day free trial HERE. Thereafter, The Pointer will charge $10 a month and you can cancel any time right on the website. Thank you
Submit a correction about this story
