

Opioid crisis kills nearly 10 Ontarians a day: Nursing Association urges PCs to change course and support overdose prevention sites
The opioid crisis—at its root—is an epidemic of an endless search for relief.
More than eight people are dying per day in Ontario due to opioid overdoses. In Canada, there were nearly 20 deaths a day between the months of January and June 2022. As many as 98 percent of these overdoses are classified as accidental.
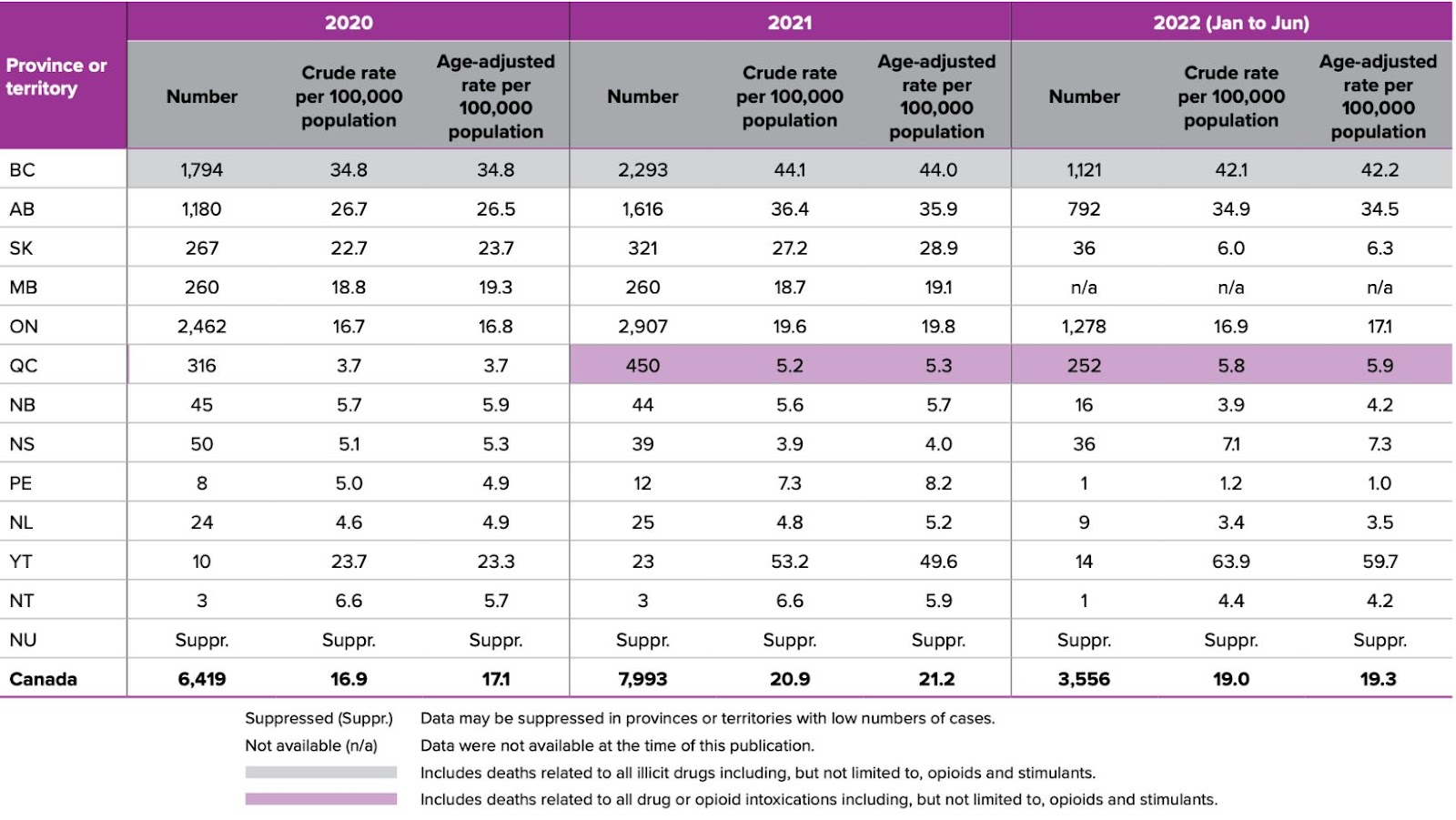
There has been a clear rising trend in the last decade which has been exacerbated since 2020.
(Health Canada)
Almost all people who use opioids were introduced to the substances unintentionally: prescribed through a medical professional for chronic pain, provided for relief after various surgical procedures, recreationally, or falling into a cycle of use while seeking a stronger high. Many of these different scenarios that lead down the path to addiction have one thing in common, the inherent need to be relieved from day-to-day life consumed by pain.
“Some people have chosen to find this way to deal with what is a concern to them and what they cannot cope with,” Dr. Claudette Holloway, president of the Registered Nurses Association of Ontario (RNAO), told The Pointer. Throughout her more than 35 years of nursing experience, Dr. Holloway has personally witnessed the explosion of the opioid crisis, which has killed hundreds of thousands of people and caused suffering of an unthinkable scale.
“People [need to] start to understand how this impacts individuals and families: there’s loss going on,” she said. “We cannot just let people lose their lives, be judgmental, and put the blame on them.”
Dr. Claudette Holloway is passionate about eliminating anti-Black racism and all other forms of racism and discrimination in nursing and the health-care system, while advancing health programs for the most vulnerable: using an equitable approach to advance nursing and health care.
(RNAO)
Dr. Holloway is adamant that harm reduction is the most effective way to mitigate the significant harms created by opioid addiction. It is one of the four pillars used in internationally recognized strategies and built from an evidence-based, patient-centred approach, using public health policies to lessen the physical, mental, and social impact of substance use. The other three pillars are Prevention, Treatment and Enforcement.
Used together, these pillars can underpin programs like education campaigns, access to free medical supplies that can temporarily prevent overdoses like naloxone, implementing Urgent Public Health Needs Sites (UPHNS) which are also called temporary Overdose Prevention Sites (OPS), and permanent Safe Consumption Sites (SCS).
With harm reduction and treatment strategies, the person using has a significantly lower chance of accidentally overdosing after taking too much or ingesting poisoned drugs because of the implementation of substance testing kits handed out through public health staff, or thanks to the presence of trained staff at an OPS or UPHNS. The pillars also feed into one another. Through harm reduction programming, users will have access to various treatment programs that can help them when they are ready to make the step toward sobriety.
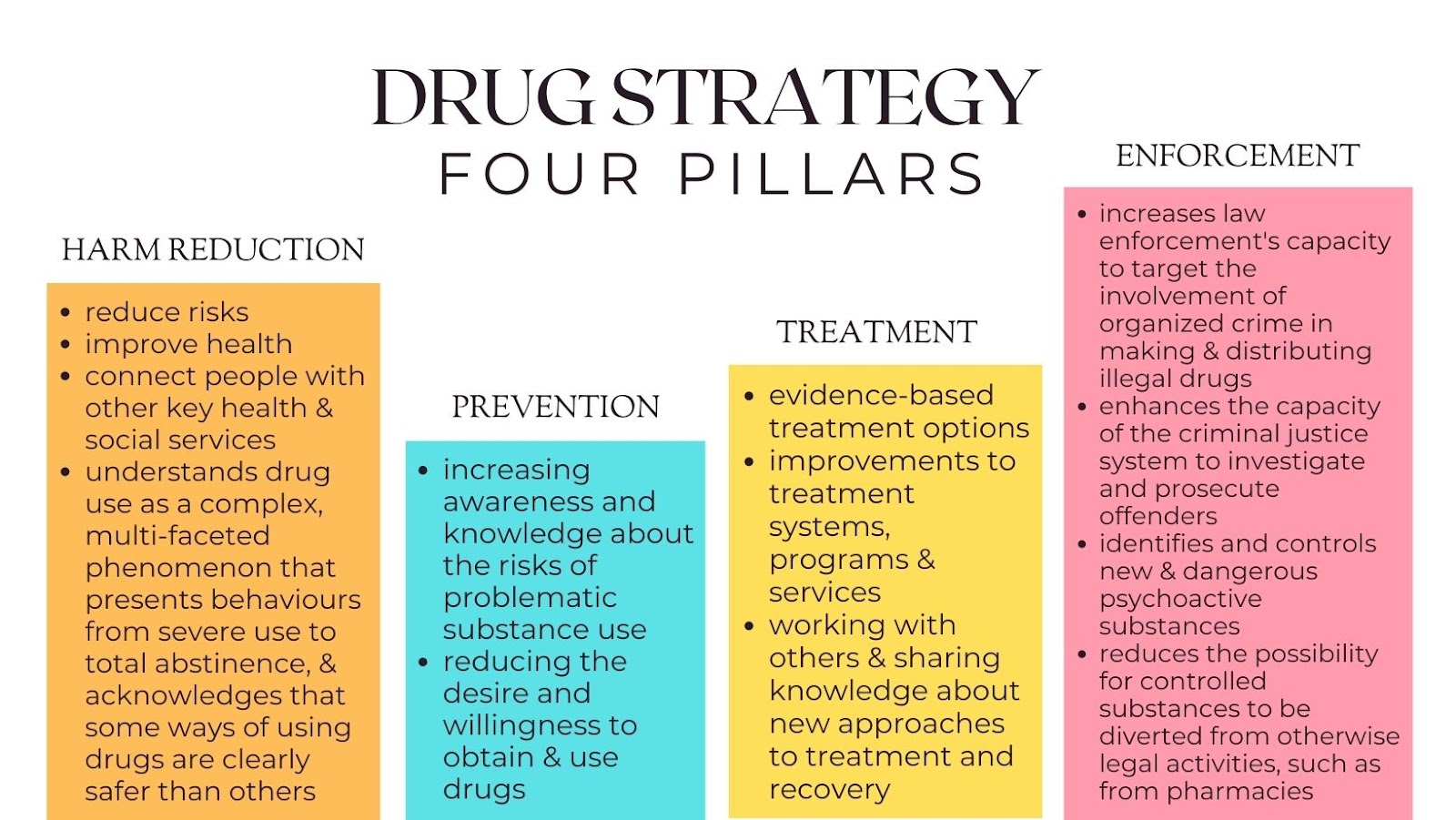
All four pillars are addressed in the Region of Peel’s Opioid Strategy approved in 2019.
(Alexis Wright/The Pointer)
In May 2022, Peel Region staff advised councillors that “immediate intervention” was needed in order to start effectively addressing the rising rates of overdoses. Two months later, Council responded with unanimous approval and immediate action to move forward with planning and implementation of a SCS—either in Downtown Brampton or Cooksville in Mississauga—at a cost of approximately $5.8 million in the first two years, with consideration for a potential mobile site that could be put into action quicker than a permanent location and start saving lives sooner.
Either site would require funding from the Provincial government.
The Minister of Health in each province or territory has authorization to establish UPHNS or SCS under an exemption put in place by the federal government through the Controlled Drugs and Substances act.
The RNAO is urging the Ontario government to take advantage of this exemption, meant to streamline the process for opening UPHNS, in order to get more harm reduction facilities operating and saving lives.
A five-year funding program available from April 1, 2018 to March 31, 2023 called the Canada-Ontario Emergency Treatment Fund (ETF) Bilateral Agreement “designed to augment treatment services through one-time funding in response to the opioid crisis” grants the ministers the funding to open UPHNS or SCS. Ontario was allocated $51,097,477.
Dr. Holloway is aware of the ETF agreement that gives the province more tools to help, but she expressed confusion on why no action has followed the promises.
“They are able to implement them, but we are still at the number of 17 that we had initially when the government came into power. We’re saying that we need more,” she pleaded.
When asked why the number of permanent Safe Consumption Sites or Temporary Overdose Prevention Sites has not increased since 2018 when the Progressive Conservatives came into power, a spokesperson for the provincial Minister of Health, Sylvia Jones, sent an email in response with a list of available permanent sites—all of them opened prior to 2018 when the PCs under Doug Ford began their first term. She did not explain why the government has failed to allow more sites to open across the province. The PC government has actually denied several applications.
“The Ministry of Health has allocated up to $31.3 million in annual funding for up to 21 Consumption and Treatment Services (CTS) in communities in need across the province. Here is the current list,” the spokesperson said.
According to Dr. Holloway, the Province promised for years to have at least 21 not-for-profit sites to effectively address the growing crisis.
“And when you go on the page that lists them, sometimes the numbers look as though they are greater, but they have repeated some sites. Also, a lot of them are privately funded,” she said.
According to the list—considering the repetition—there are only 16 sites in Ontario.
However, on the government of Canada’s list of services there are 24 in the province.
A spokesperson for the federal Minister of Mental Health and Addictions, Carolyn Bennett, said the government of Canada has invested more than $800 million since 2017 in a wide range of actions and interventions to address the [opioid] crisis, help reduce the stigma surrounding substance use and meet the diverse needs of people who use them.
“This includes funding for community organizations, safer supply projects, public education campaigns, approving supervised consumption sites and increased access to culturally appropriate, trauma informed, and evidence-based treatment and supports,” she said.
“Since that time, the number of supervised consumption sites across Canada went from 1 to 38—24 of which are in Ontario—and they have been visited more than 3.9 million times, reversed over 43,000 overdoses, and made over 214,000 referrals to health and social services.”
The actual number of sites is lower than what is listed because, in some cases the same location involves multiple licenses to offer different services such as for a SCS as well as an inpatient stay facility, so the site might be listed twice on the list.
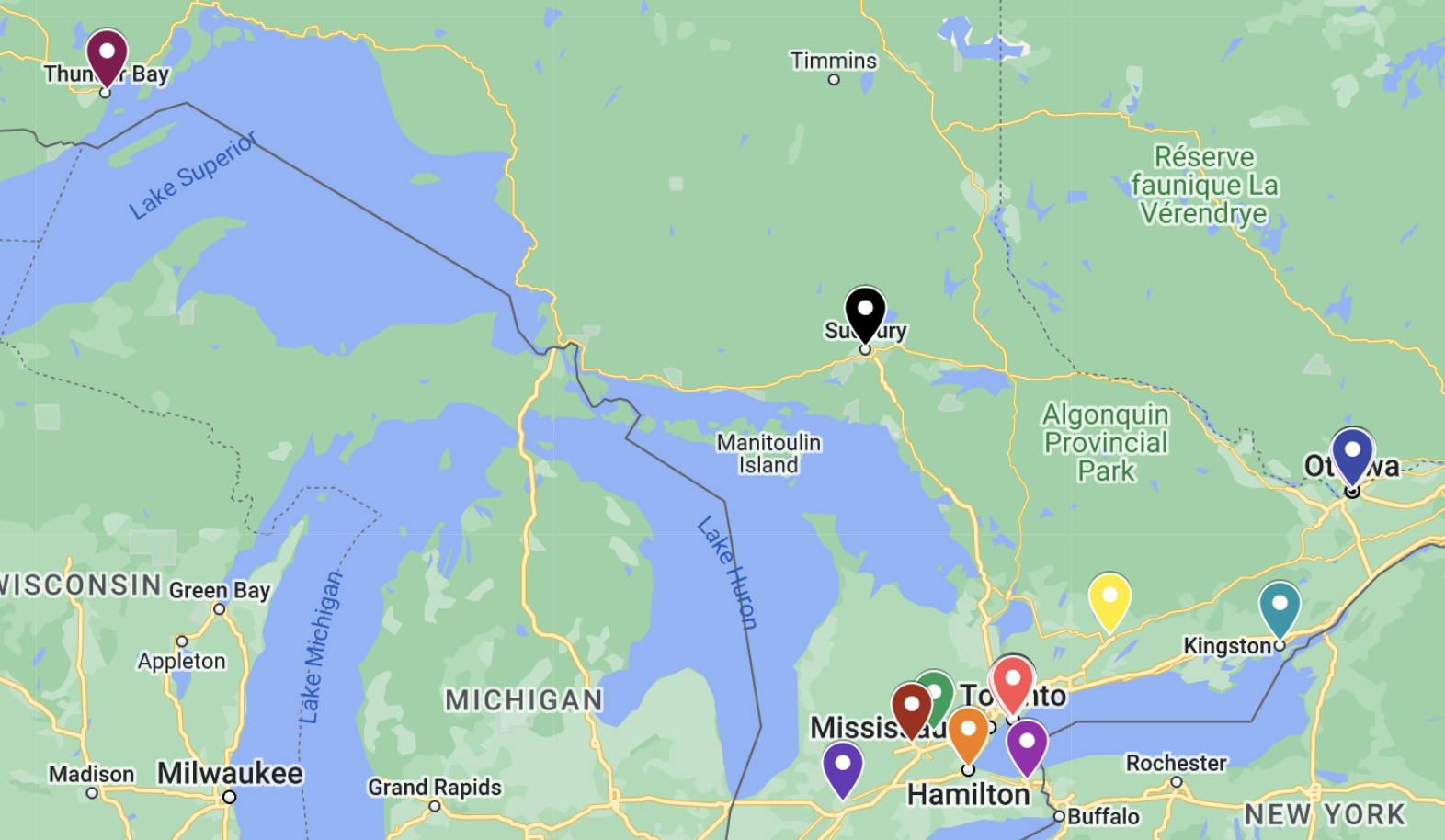

Those seeking support within the Region of Peel currently have to travel out of their city to either Toronto with very long wait times or Guelph where there are fewer available services.
(MyMaps/Google Maps)
“The bottom line is: the federal government needs to do more to help the opioid crisis. They want to eliminate it because we want to save lives,” Dr. Holloway said. “So we need that funding that would guarantee that we would have a safe supply, and so that drugs can be checked, also the decriminalization of possession because it’s not a criminal matter—it’s a health matter.”
The federal government says it is the responsibility of the Province to make the final determination.
“It is the Minister of Health's discretion if they wish to implement the class exemption or not. Currently, Ontario is not using the class exemption. If the provincial Minister of Health is not establishing any urgent public health need sites in the province or territory, sites may apply to Health Canada to set one up,” the spokesperson for MP Bennett told The Pointer.
Nine of the sites are operating under a federal exemption in Ontario without help from the provincial government.
Since 2017, Ottawa has invested $5.3 billion over ten years, with multiple envelopes to increase access to mental health services, address the mental health needs of marginalized and disproportionately impacted residents and support health system improvements.
Through Budget 2022, they also funded the Wellness Together Canada portal providing residents with tools and services to connect them to cognitive behavioral therapy support, child and youth mental health services, addictions services, supportive housing and mental health practitioners.
As per the Ontario Action Plan, the province planned expenditures from 2018 to 2020 toward “enhancing existing treatment approaches at the local level, expanding support for culturally appropriate care, and implementing strategies to enhance access to treatment through integrated services at Consumption and Treatment Services sites”.
The Pointer asked Jones’ spokesperson about how the ETF has been implemented over the past five years—considering no new UPHNS have been opened by the province—but the question was not addressed.
“We think other things take their priority yet we want to make sure that they understand that every life is important. And while they are dealing with other things, we cannot let this crisis go unnoticed,” Dr. Holloway said.
It’s clear that if more action is not taken, lives will continue to be lost, especially after COVID-19 exacerbated many of the preexisting issues affecting the drug-using population.
The COVID-19 pandemic has had severe impacts on the crisis worldwide. On top of the negative stigmas often associated with drugs that cause more feelings of shame for some users, the isolation often forces people to use alone when the risk of death is at its highest.
“We know that the death rate has doubled since the pandemic. It hasn’t quite settled yet,” Dr. Holloway said.
“There’s so much stigma around opioids that [users] continue to hide. If we can get more of the safe injection services, then they can come out and we can start to see the number go down. But we don’t want to see it continue to escalate at the rate that it’s going. It’s not acceptable.”
British Columbia has recently started a pilot project that decriminalizes illicit substances. People can travel with 2.5 grams of the substances included in the program to and from the centres without the risk of being stopped, fined, charged or arrested for carrying a substance otherwise currently deemed criminal.
“That’s why they’re staying put,” she asserted. “They need that protection that would say they can safely go with that 2.5 grams or less so they can access the care they need.”
Experts say that until decriminalization is mandated across the country, changing widely held perceptions, UPHNS likely will not operate to their full potential because many fear being arrested while carrying a substance on the way to access support. Vulnerable populations could be uniquely impacted as they are at a higher risk of interactions with police due to systemic racism and discrimination that has plagued law enforcement for decades, while other dimensions of institutionalized bias across society compound the suffering many can’t escape.
Criminal charges come with many risks, one being feelings of contempt or disillusionment for innumerable reasons which quietly push in on users who lose the motivation to seek help. Too often, these feelings of helplessness or anger lead to tragic consequences.
“These days it’s so hard to cope with what is going on,” Dr. Holloway said. “A lot of people are not aware, they’re just trying to meet their own needs. It’s not like they’re intentionally going out and trying to harm themselves, mostly they're just trying to deal with whatever they’re trying to manage in terms of their own grief or trauma. So it's the responsibility of our healthcare system to put resources in place to deal with these things.”
The lack of access to resources, low wages and precarious living conditions in a historically unaffordable housing market can create unbearable pressure, triggering deep feelings of hopelessness or despair. Drugs can offer a false sense of escape, a brief respite from the pain. Infrequent use often bleeds into occasional use and then, with little control of external forces, a darkly dangerous habit grips users as the underlying pressures grow heavier and heavier.
Without broad societal solutions to many of the problems created by poor policies, inequitable funding and relentless racism, gender discrimination and discrimination based on sexual orientation, along with a range of other avoidable contributors, the need for support will only grow. Meanwhile, the long-term effects of using substances in the absence of these supports, only makes the suffering worse. Neglecting the need today for more funding outside of the emergency fund, to create permanent mental health supports, will make things much worse tomorrow.
“In that broader context, we need that access to mental health support so people dont feel that stigma and they can come out in the open to say ‘this is how I’ve chosen to deal with it and let me have some resources and I’ll make the decision.’ There’s a whole number of things involved, like mental health is a huge aspect that we still need the government to do so much more about. Why are we still treating this as a criminal offense?” Dr. Holloway questioned. “This is a health crisis.”
In the mental health sector, the Ontario government has invested a total of $525 million in base funding since 2019 to begin addressing the growing need for support under its Roadmap to Wellness plan: $130 million for child and youth mental health; over $80 million for community mental health, including investments in Ontario Structured Psychotherapy; $93 million for addictions treatment services and supports, as well as an additional $9.05 million for youth wellness hubs; and $16.6 million for services and supports for treatment for children, youth and adults with moderate to severe eating disorders.
The Ontario Psychological Association (OPA) released a statement on January 23 that Ontarian's demand for mental health services rose over 50 percent in 2022, and because the increased demand means even longer wait times for public services, residents are seeking private services more often.
Countless statements released since 2018 claim the provincial Ministry of Health has been taking action to address this crisis, pointing out repeatedly that these available services would be covered under OHIP.
When asked what the Ontario government is doing to address these wait times and the push to private services, Jones’ spokesperson responded by listing one-time investments.
“Additionally, our government is implementing the Addictions Recovery Fund, a one-time investment of $90 million over three years to boost capacity in addictions services,” she wrote.
An increasingly common way to access opioids is through drug trafficking which has been proven to disproportionately affect Indigenous peoples and other vulnerable populations.
"Women who use drugs face consistently higher barriers to harm reduction services than men, and there is a lack of services specifically tailored to women’s needs. Pregnant and parenting people face particularly acute stigma and discrimination when accessing harm reduction services, despite all evidence indicating that parental substance use is best addressed by harm reduction," the Global State of Harm Reduction 2022 report explains.
Despite representing less than 3 percent of the total population, Indigenous peoples account for 10 percent of fatal overdoses.
According to a study in the Canadian Medical Association Journal, Indigenous women are five times more likely to experience a fatal overdose than non-Indigenous women. "The severity of this crisis is likely understated owing to poor disaggregation of data on Indigenous Peoples in many settings,” the research published in 2018 states.
These substances make their way across borders (often with illegal firearms and significant sums of cash) and flood city streets faster than public health and law enforcement are able to respond.
More and more prevalent in police busts is the presence of the synthetic opioid fentanyl. In 2022, fentanyl was present in 34 percent of overdoses in Canada.
On February 1st, Toronto Police released a statement about the completion of Project Cerro. They seized an estimated $32 million (street value) of drugs: 364 kilograms of crystal methamphetamine, 20 kilograms of cocaine, and 3.8 kilograms of fentanyl—enough of the synthetic substance to kill more than 300,000 people.

Effective March 27, 2018, participating pharmacies provide naloxone (Narcan) nasal spray kits that temporarily reverse an overdose. Eligible recipients do not have to have an Ontario health card number or identification.
(The Pointer Files)
It’s not just the streets that are a concern, flaws in the healthcare system have been ignored for decades.
“Of course there's the overprescribing that has been going on for years,” Dr. Holloway said.
There are no platforms currently in place to link an individual’s medical records for any doctor or other professional in the medical field to review when medication is sought in a range of settings. This creates a dangerous environment for patients to abuse Ontario’s current health system. A person seeking relief can go from clinic to clinic with the same complaints of pain and documentation of a previous diagnosis, warranting a prescription for the type of medication they ask for.
Dr. Holloway, like many advocates, said a comprehensive national system is badly needed to link everyone’s records virtually, triggered simply by inputting a health card number at the beginning of the visit, while chronic visits to clinics and pharmacies could be flagged by the system.
Just before the October municipal election, the RNAO held a campaign to talk to mayoral candidates and leaders of municipal government so they could better understand their role in dealing with the opioid crisis. They were asked to sign a pledge.
“Not all of them signed on to say ‘yes, we intend to do something about it’. We really need to get everyone on the same page and help them to understand. But some of our decision makers choose not to see those kinds of barriers and stigmas that are the reality of some of the population they’re elected to serve. And they’re elected to serve everyone,” Dr. Holloway said.
Neither Mayor Patrick Brown nor Mayor Bonnie Crombie signed the pledge.
“Elected officials are responsible to provide access to everyone and that was the challenge we brought before them but not everyone was willing to sign on,” she said.
“Still, we brought attention to that issue, we brought it to the forefront—so at least they can't say that they haven’t heard of it.”
Canadians will continue to lose their lives unless intervention is implemented as soon as possible.
On Tuesday, Prime Minister Justin Trudeau announced a proposed ten-year, $46.2 billion deal with the provincial and territorial leaders of Canada to expand the annual health transfer that funds our universal system across the country. Premier Doug Ford was among many of the premiers who was disappointed with the sum, representing the overall increase to the transfer which will be divided between the provinces and territories based on population.
Unless the funds are allocated effectively, experts say increasing the amount will not have the same effect on the multi-level healthcare crisis crippling hospitals and other facilities across the country.
There have been few details about how the federal government and the provinces might negotiate allocation of the increased healthcare funding. It remains unclear if desperately needed investments in mental health support and programs to address addictions, along with safe injection sites and overdose prevention sites will materialize from Ottawa’s expanded health transfer.
Since June 2022, there have been no requests from Jones to use the existing five-year Emergency Treatment Fund which expires in just under two months, and it remains unclear if Ontario’s PC government will prioritize the opioid crisis when it decides how to use the extra billions from the federal government.
“The politics of what comes first and what comes second is not really the focus we want, we want them to focus on saving lives,” Dr. Holloway pleaded. “We want that safe space for them to access healthcare, education, and counseling that they need.”
Email: [email protected]
Twitter: @lextoinfinity
COVID-19 is impacting all Canadians. At a time when vital public information is needed by everyone, The Pointer has taken down our paywall on all stories relating to the pandemic and those of public interest to ensure every resident of Brampton and Mississauga has access to the facts. For those who are able, we encourage you to consider a subscription. This will help us report on important public interest issues the community needs to know about now more than ever. You can register for a 30-day free trial HERE. Thereafter, The Pointer will charge $10 a month and you can cancel any time right on the website. Thank you
Submit a correction about this story
