

UPDATED: A COVID watershed—Case counts don’t mean what they used to, but risks can’t be taken with the public’s health
This article was originally published December 30, 2021 and was updated Monday, January 3.
In early 2003, as Toronto became the western world’s epicentre for the spread of SARS, many of the headlines dominating the public conversation reflected the intense focus on the economic, not the medical consequences of the deadly disease.
"We are talking... millions of dollars in lost potential (economic activity)," former Toronto councillor Joe Mihevc told CBC Newsworld on April 20 of that year.
Under increasing pressure from the business community, the travel industry, Pearson Airport officials and local politicians, the most crucial public health restrictions, imposed shortly after the outbreak began, were lifted on May 17, 2003, just three months after Toronto’s first known case.
“The real driving force of letting some of these guidelines be relieved," Dr. Mark Cameron told This American Life last year, "was the economic pressure of having a city like Toronto almost shut down trying to deal with an infection like this.”
Cameron is an Ohio-based academic who teaches genetic epidemiology at Case Western Reserve University and was on the frontlines during the 2003 SARS crisis as part of a rapid research response team while doing post-doctoral work in Toronto.
He witnessed what happened next.
Despite widespread relief that the economy had been spared any serious damage, there was little concern expressed among local public health officials and politicians about the possibility that SARS was still lurking.
It was.
They were wrong.
The tragic irony, after the loss of 44 Canadians, mostly in Toronto, to the disease, was that the economic fallout was probably ten times greater because of the premature lifting of restrictions. It was estimated that SARS, by the time the virus had been truly controlled in 2003, eventually cost the Ontario healthcare system and the Toronto economy about $2 billion.
The rapid rise of the now dominant Omicron variant of SARS-CoV-2, has put the latest debate between extreme public health measures and less restrictive responses into motion again.
We are at a watershed in the pandemic.
On Monday, January 3, Premier Doug Ford and other provincial officials announced sweeping new restrictions to confront the rapid spread of Omicron. Schools will be closed for in-class learning with virtual education in place until at least January 17, and indoor dining in restaurants has been temporarily halted. A number of other measures were also taken to slow down the viral spread, as hospitalizations and ICU admissions rise, while staffing shortages have hit health care systems across North America, as Ontario and other jurisdictions struggle with widespread problems due to burnout, resignations and illness among frontline healthcare staff.
Ford repeatedly said admissions and ICU numbers are now being carefully considered as staffing issues and infection levels threaten to overwhelm hospitals.
With widespread vaccine protection in countries like Canada, the question has shifted to what future public health responses should be based on.
More and more doctors, epidemiologists and virologists have made it clear in recent weeks that rising case counts need to be viewed in a different context than they were a year ago.
Early data from the United Kingdom and South Africa suggest the new variant could lead to significantly less severe outcomes than previous viral spread during the pandemic. The recent information also shows Omicron has a much higher rate of transmission compared to earlier variants of the novel coronavirus, which has led to a rapid rise in new daily cases in many countries around the world.
The new threat is posing a dilemma for public health officials and politicians.
Without a clear idea of what the data in Ontario will eventually reveal, should there be a worst-case-scenario response, or a more tempered reaction that considers factors such as widespread vaccine protection, the possibility of less severe disease caused by Omicron and the need to contemplate more of an epidemic reality rather than a never ending pandemic?
“As Omicron Hits, COVID-19 Case Counts Don't Mean What They Used To”. That was the headline in Time magazine two weeks ago. The two American medical professors who authored the piece, Dr. Monica Gandhi and Dr. Leslie Bienen, each with a background in infectious diseases, wrote, “We have reached a point in the pandemic where policy should no longer be based around the idea that we cannot resume normal life until case numbers are below a particular (arbitrary) level. One reason is that those levels were set before vaccination, and have not been adjusted accordingly, even though a large proportion of cases, in part due to the growing proportion of cases that are breakthrough cases, are now mild. Another reason is that these metrics were set at a time where policy makers were scrambling to set thresholds to open and close social institutions in the absence of robust data. Setting thresholds for activities according to cases no longer makes sense…”.
In a letter this week signed by more than 500 Ontario doctors, requesting Queen’s Park keep schools open, the physicians said, “School closures should no longer be a knee-jerk reaction to rising case counts. Numerous jurisdictions have committed to keeping schools open and we need to do the same.”
Instead of case counts—which capture everything from completely asymptomatic individuals to those with severe disease, and everyone in between including many reporting symptoms milder than the common cold—data such as ICU admission rates, hospitalizations and other indicators of more serious disease need to dictate policies going forward, experts say.
In its latest presentation on December 16, Ontario’s Science Table suggested a brief lockdown should begin immediately. The advisory group said contacts must be reduced by 50 percent in order to “blunt the Omicron wave”, also calling for an increased emphasis on air filtration and high-quality masks.
The experts that make up the advisory body admitted there was a lot they did not know about Omicron — and there still is.
After two years of healthcare chaos, the Science Table argued it was better not to wait for the telling data. “Although uncertainty persists, waiting for more information will eliminate the opportunity for action,” a slide from the Table’s presentation reads.
The experts presented two scenarios: one where Omicron is more transmissible than the previous Delta variant of COVID-19 but equally severe, and another where it is 25 percent less severe. The former scenario saw intensive care unit occupancy rise to as high as 600 patients in Ontario by the New Year and the latter modelled a maximum of just below 500.
Some of the early data suggests reason for optimism.
On December 29, according to data from the provincial dashboard, there were 176 people in intensive care who had tested positive for COVID-19. The number represents a 21 percent increase in ICU occupancy from December 19 and a marginally better outcome than even the most optimistic modelling done earlier by the Science Advisory Table.
In Peel, the latest data show there were 3,977 new infections in the 14 days up to and including December 23. But the current hospitalization numbers are much lower than they were during the peak of a wave one year ago, and during the high-point of the spring wave.
The seven-day moving average for daily hospital admissions for those with COVID-19 show three new patients were being given a hospital bed in Peel each day, as of just over a week ago. The Region’s December 24 weekly report shows “22 currently admitted” COVID patients in Peel hospitals.
These figures compare favourably to the data in the same weekly report from about a year ago, when daily case numbers were near the peak of the wave that hit ahead of last year’s holiday season. The December 18, 2020 report showed a seven-day moving average of 10 daily admissions of COVID patients in Peel hospitals, and “138 currently admitted” covid patients at that time.
While there were 1,077 new cases reported on December 23, just a week ago, one of the highest single-day figures yet, according to Peel Region’s dashboard, it’s not clear if the current wave is nearing its peak, or how long it will last, as early indications from other countries suggest the Omicron wave comes and goes much faster than previous waves.
Because the current data is based on a much shorter curve to the recent case count numbers, and with the possibility that we are not yet at the peak of the Omicron wave, the two sets of figures should not be considered an apples to apples comparison of each wave, but rather a point in time comparison.
By mid-to-late January there should be enough data, and any possible lag period should no longer skew the numbers, allowing officials to determine if ICU and hospital admissions (not daily case counts) along with other medical indicators warrant more severe policies.
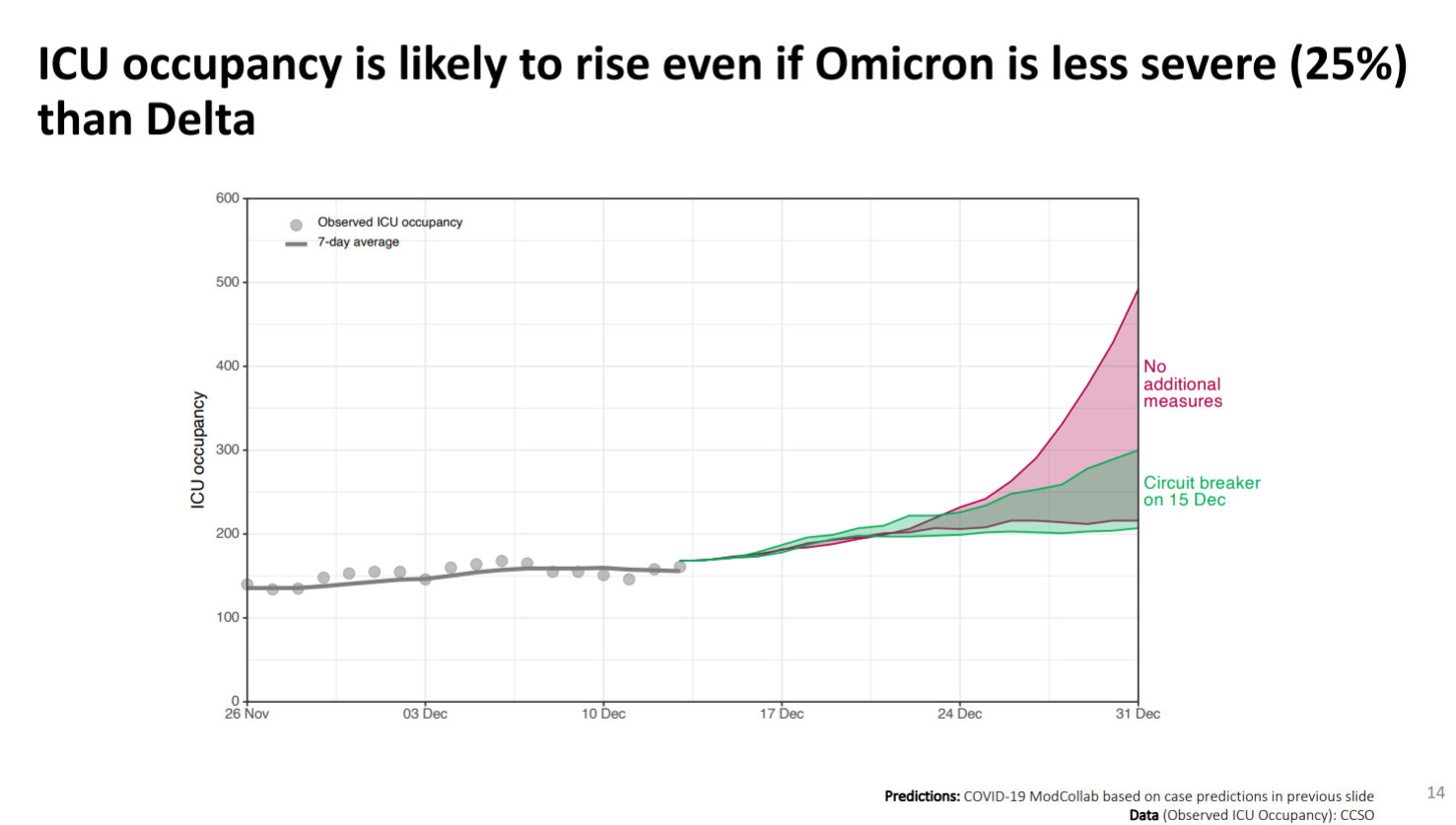
The Ontario Science Table suggested a circuit breaker and feared that even if it was less transmissible, Omicron could pose a grave threat.
(Image from Ontario Science Table)
The number of people in hospital as a result of COVID-19 is significantly lower than during the worst periods of Ontario’s wave in January or the wave in April.
It is unclear if Omicron is peaking in Ontario and just how high it might go. South Africa, where Omicron was first identified in November, appears to be on the downward slope of its wave, while the United Kingdom, which has generally been a few weeks ahead of Canada’s COVID-19 situation, was still on a rapid upward trajectory one week ago, with daily case numbers not seen since the start of the pandemic.
Peel Region, which was battered during the early waves of the pandemic, now has one of the best vaccination rates in Ontario and no longer leads daily case counts, putting it in a more favourable position as Omicron spreads. Residents 12 years and older in Peel have the eighth highest vaccination rate of Ontario’s 34 public health units, ahead of Hamilton, Toronto, York and Waterloo.
Eighty-seven percent of Peel’s residents five years old or above have received at least one dose and 82 percent are fully vaccinated. Out of those 12 years old and above, 92 percent have received at least one dose and 89 percent are fully vaccinated.
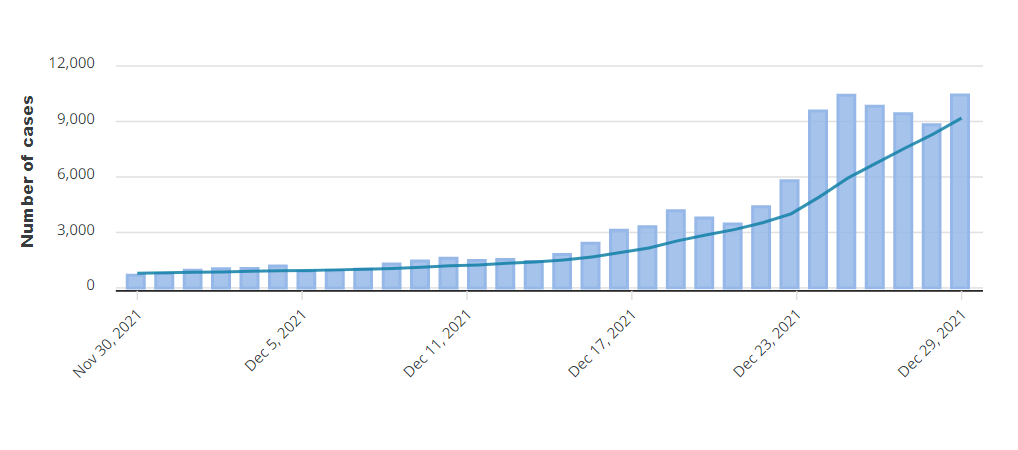
Ontario’s average daily case count has continued to rise throughout the holidays.
(Screenshot from Government of Ontario)
In the last three weeks, Peel’s hospital capacity has remained consistent, and as of December 20, 71 percent of ICU beds were filled, but only 43 percent of those with ventilators were occupied.
Acute care beds in the region’s three hospitals remained at 100 percent capacity, but this includes non-COVID patients as well.
About a year ago, as of December 14, 89 percent of ICU beds in Peel were occupied and 66 percent of those with ventilators were being used.
It’s possible that if the current wave worsens, Peel’s hospitalization, ICU and ventilator capacity could also worsen, as even those who are vaccinated can still get very sick, particularly patients who are older or have underlying conditions.
“We had a case surge last week and are seeing close to an average of 900 cases per day,” Monica Misra-Lui, a spokesperson with Peel Region, told The Pointer Wednesday. “With hospitalization as a lagging indicator by approximately 2 weeks, we continue to monitor to see the impact of Omicron on hospitals. We’re also closely following other jurisdictions worldwide as well as more locally (e.g., Kingston).”
Whether or not Omicron continues to spread at a faster rate and more daily cases are seen in Peel, the next two to four weeks should indicate if disease is more or less severe, or roughly the same, compared to earlier waves, and what the actual impact on the healthcare system is now that so many Peel residents are vaccinated.
Data from the Ontario Science Table, reflected in other jurisdictions around the world, show serious outcomes are more common among those who are yet to be vaccinated. Of Ontario residents currently hospitalized with COVID-19, 17.3 out of every million double-vaccinated Ontarians are in hospital, compared to 221.3 unvaccinated residents. This shows the rate of hospitalization is about 13-times higher among the unvaccinated.
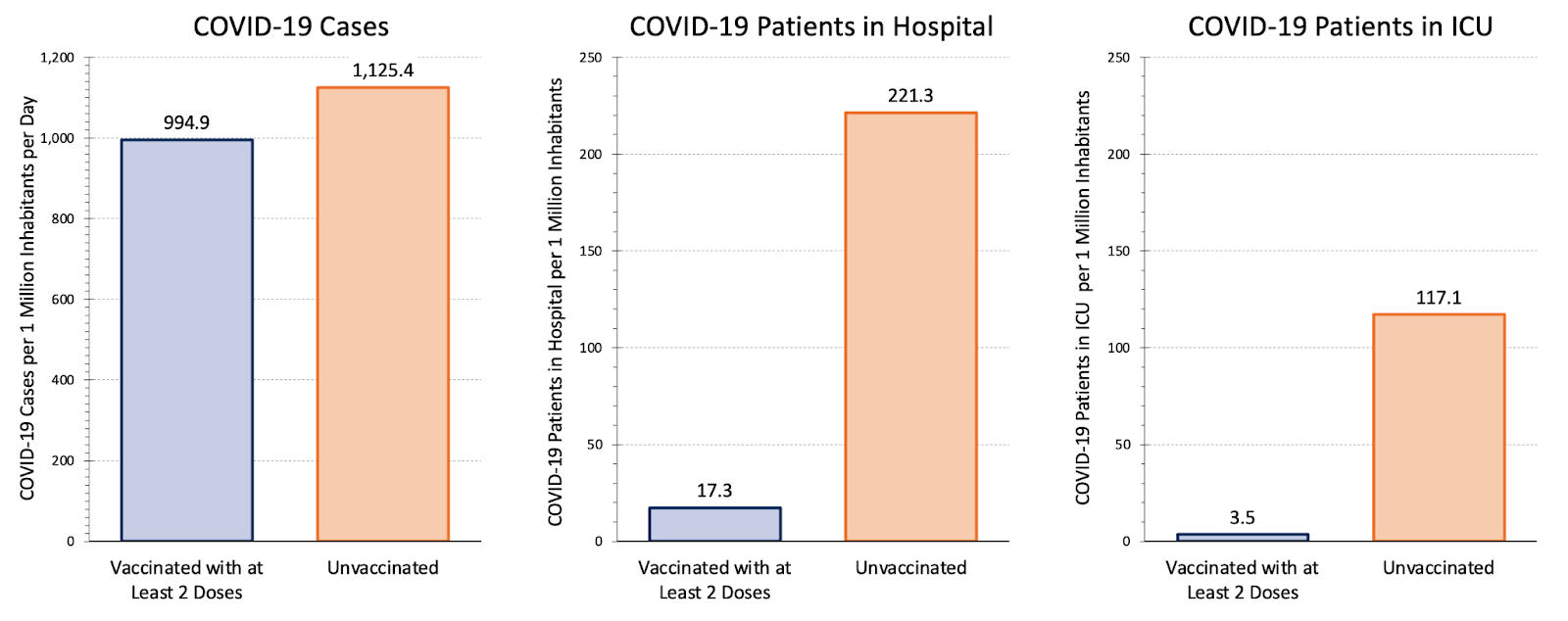
Data from the Ontario Science Table shows the protection offered by vaccines.
(Image from Ontario Science Table)
Ontario’s Omicron wave compares favourably to the province’s previous waves, at least so far. Data from the peak of the wave in mid-January and the next wave in late-April show that a significantly higher proportion of active cases around Ontario resulted in hospitalizations.
Between January 7 and 20, the province averaged 28,746 active cases every day, with an average of 1,578 people in hospital with COVID-19. The next peak, from April 15 to 28, saw an average active case count of 41,072 cases per day and 2,206 people in hospital. During the January peak, around 5.5 percent of active cases were in hospital, dropping marginally to 5.4 percent in April as vaccines began to kick in.
While it is unclear if the Omicron wave is peaking, the early data in Ontario looks promising. The number of active cases on average in the two weeks leading up to December 23 (before holiday schedules began to impact reporting) is lower than the previous two peaks.
From December 10 to 23, there was an average of 17,487 active cases in Ontario. Active cases increased 253 percent during that time from 9,193 to 32,412 and continue to rise. Hospitalizations, however, are markedly lower, but are showing signs of gradually increasing. On average over the two weeks preceding Christmas, there were 342 people in hospital, roughly 2.2 percent of active cases. This figure is less than half the hospitalization rate of previous waves.
The age of COVID-positive patients is a factor that also differentiates the various waves in Ontario.
On January 7, almost a year ago, 5.6 percent of all COVID-19 tests for those 65 years and older returned a positive result, rising to 5.9 percent during the next surge on April 18. So far, a test positivity rate of 3.7 percent on December 16 is the test positivity peak among older Ontarians during the current wave.
The distribution of cases between age groups is one factor, along with vaccination and the severity of Omicron, that could impact hospitalization data, helping reveal how serious COVID-19 might be going forward, in a widely inoculated population. Even more and more individuals who are not vaccinated will develop natural immunity as an increasing number of them are infected.
Initial data from the United Kingdom holds hope the current variant is less damaging, especially in well-vaccinated populations.
“These early national data suggest that Omicron is associated with a two-thirds reduction in the risk of COVID-19 hospitalisation when compared to Delta,” a pre-print study on Scotland’s Omicron wave from the University of Edinburgh says.
There are differences in how Ontario reports its data compared to the Scottish study, but the central message is positive. Work relied upon by the University of Edinburgh defined a COVID-19 hospitalization as someone who tested positive within 14 days prior to their admission to hospital or two days after being taken in. Ontario, by contrast, currently tracks this metric as well as cases that were in hospital prior to acquiring the disease.
Travis Kann, deputy chief of staff for strategic communications to the Premier of Ontario, confirmed Ontario will begin asking hospitals to differentiate between those in hospital as a result of COVID-19 and those who incidentally tested positive.
Different countries and leaders have approached the changing threat of Omicron in a variety of ways.
In the Netherlands, a strict lockdown was brought into place before Christmas because inaction would lead to an “unmanageable situation in hospitals”, Dutch Prime Minister Mark Rutte said. Until at least mid-January, non-essential shops, gyms and hairdressers will be closed, while a limit of two guests in private homes will be allowed.
By contrast, British Prime Minister Boris Johnson has resisted calls for major new restrictions. Some rules, such as masking indoors, have returned after a brief hiatus in England, but New Year parties and sold-out sports stadiums look set to continue in England.
Sir John Bell, regius professor of medicine at Oxford University and the British government’s life sciences adviser, has said Omicron “appears to be less severe and many people spend a relatively short time in hospital”. Speaking on BBC Radio 4, he said: “The horrific scenes that we saw a year ago of intensive care units being full, lots of people dying prematurely, that is now history, in my view, and I think we should be reassured that that’s likely to continue.”
Others have warned that, even if hospitalizations are lower and Omicron ultimately proves less severe, there could be major repercussions to inaction as a result of how easily the virus spreads. Professor Alison Leary, chair of healthcare and workforce modelling at London South Bank University, has warned that 40 percent of National Health Service staff in London could be absent through illness in a worst-case scenario. The UK’s Rail Delivery Group said that in the seven days leading up to December 24, an average of 5.4 percent of trains were cancelled, compared with the annual rate of 2.9 percent.
Stricter measures have been introduced in both Scotland and Wales.
The Centers for Disease Control and Prevention (CDC) in the United States has recommended a shortening of the quarantine period for those exposed to COVID-19 and people who test positive but remain asymptomatic.
How this all impacts Ontario and Peel is unclear.
A range of responses to Omicron and its early data around the world show politicians asserting a range of governance styles. A move away from case counts as a key measure is being embraced in some jurisdictions, with critics reminding leaders that hospitalization data has always been a lagging indicator.
Expert opinion itself is also beginning to diverge. The letter signed by more than 500 doctors in Ontario asks Premier Ford to keep schools open in the New Year, as parents wait anxiously to find out if new restrictions may land just days before children are supposed to return to the classroom.
The decision that Ford and his cabinet make next will be a big indication of policy going forward. So far, both Queen’s Park and Ottawa seem to be on the fence, issuing advisories instead of orders and smaller restrictions rather than lockdowns. Monday's moves further indicate a balance between past public health considerations and the need to contemplate other factors, including mental health.
The next two to four weeks of hospital data should tell us which direction policy needs to move in.
It’s a true dilemma.
No one wants a return to lockdowns.
But no one wants a repeat of the 2003 miscalculation on SARS, which turned out so tragically.
Email: [email protected]
Twitter: Anukul_AT
Email: [email protected]
Twitter: @isaaccallan
Tel: 647 561-4879
COVID-19 is impacting all Canadians. At a time when vital public information is needed by everyone, The Pointer has taken down our paywall on all stories relating to the pandemic and those of public interest to ensure every resident of Brampton and Mississauga has access to the facts. For those who are able, we encourage you to consider a subscription. This will help us report on important public interest issues the community needs to know about now more than ever. You can register for a 30-day free trial HERE. Thereafter, The Pointer will charge $10 a month and you can cancel any time right on the website. Thank you
Submit a correction about this story
