

‘They're leaving every day’: Peel Nurses giving up on profession, especially after PC’s wage suppression law
Nursing shortages are not new to Ontario.
Since the ‘90s, the number of nurses per 100,000 residents in Ontario has almost always been behind the national average.

Ontario lags behind the nurses per 100,000 residents in Canada.
(RNAO)
“In the past, we did have a shortage of nurses, but it was never to the extent where we are now,” says Mary Aubin Cadet, a registered nurse who has spent over 20 years in patient care.
She says the lack of nurses in Peel, where the population increase outstrips the public sector’s ability to keep up with rapid growth, is not new but new-age problems are exacerbating the shortage.
“The salary cap is not increasing and it is not worth it for people, especially for community health,” Cadet says.
The ongoing pandemic which is receding but not completely retreating, has caused a profound impact in the nursing profession around many parts of the world. In places where the toll has been far more severe than any health crisis previously experienced, many nurses have simply been ground down, beyond the point of being able to provide needed care.
Call it compassion fatigue or a loss of the ability to work empathetically, these frontline healthcare warriors have been betrayed by a system that has placed a horribly overwhelming burden on their shoulders.
Few could endure what many nurses have been forced to do for almost two years.
Some of the cascading pressures have only made things worse.
Staffing shortages in homecare nursing became worse because there is no guarantee of sustained income in homecare and many left to work in long-term care, Cadet says.
“That meant more work for the nurses that chose to stay and long hours meant the workload was heavier.”
Homecare nurses like Cadet had to shoulder additional stress during the pandemic.
“It was very, very, very overwhelming and stressful and when you see everybody around you panicking, you can’t keep calm.”
She says what hospital-based nurses continue to face is similarly overwhelming but one advantage they have is the insulation of layers of healthcare and support that surround them. “At the hospital you're in an institution”, but when you go to your client’s home, you are on an island, she says.
“We take care of the client physically, psychologically, mentally, we are the backbone of healthcare and I hope the government and the other population can understand that.”
Paula Manuel has been a registered nurse for the past 40 years and COVID-19 isn’t the first pandemic she’s seen.
“I lived through SARS. SARS was the first real inkling that nurses were not always listened to because we didn't say things in a popular way,” Manuel says.
“Archie Gray Campbell, former Justice of the Superior Court of Ontario, said ‘Even if you don't agree, if the workers tell you that there's something wrong, you should listen to them’.”
“So here we are in the pandemic but nobody is listening again.”
Before the pandemic hit, Manuel had moved up to a management role and when the virus arrived her job involved directly supporting her colleagues working on the frontlines.
“I was restructured, we had a list of people that were my circle that I would follow every week and listening to their stories was my contribution because it was absolutely humbling to hear what they were going through, the hours that they were working,” she says.
Nurses are burnt out, and the Ford government's wage cap is only exacerbating their stress.
(RNAO’s Ontario's RN Understaffing Crisis Report (RNAO))
Manuel says it was the nurses who made sure others had the protective gear on before anyone would step inside a room with a COVID positive patient.
She recalls one of her friends say, “I felt like a mother’s hand when I got my first fastener stressed to go into a Covid-19 positive patient - I would double check, triple check all the ties make sure that the visor was on correctly, the eye protection, the mask was on all our stuff.”
The pandemic changed the code that nurses practiced as well. Before, everybody would go into the room to help a patient in distress.
“If someone was not breathing well, if someone had a seizure, or if their heart was not working, everyone would cycle through with CPR but to cut down on the exposure to the coronavirus the emergency procedures changed.”
“With COVID-19 practices, there was a cohesive unit of a doctor, a nurse and a respiratory therapist—that's it.”
Navjit Kaur has been a respiratory therapist at the Brampton Civic Hospital for almost a decade but 2020, unlike any other year, left Kaur herself gasping for air.
“Our main goal is to help someone breathe. If a patient is in the ICU, if they're on a ventilator, we intubate, we do Arterial Blood Gasses (ABGs)—we help them breathe.”
With the pandemic, Kaur did not know what to expect.
“My colleagues were just telling ourselves, okay, just breathe, you'll be fine. You just go in and just breathe,” she says.
“Even though you were in full PPE, after seeing how difficult it was for these patients to breathe, not even knowing if they would make it the next day, you are scared and stressed.”
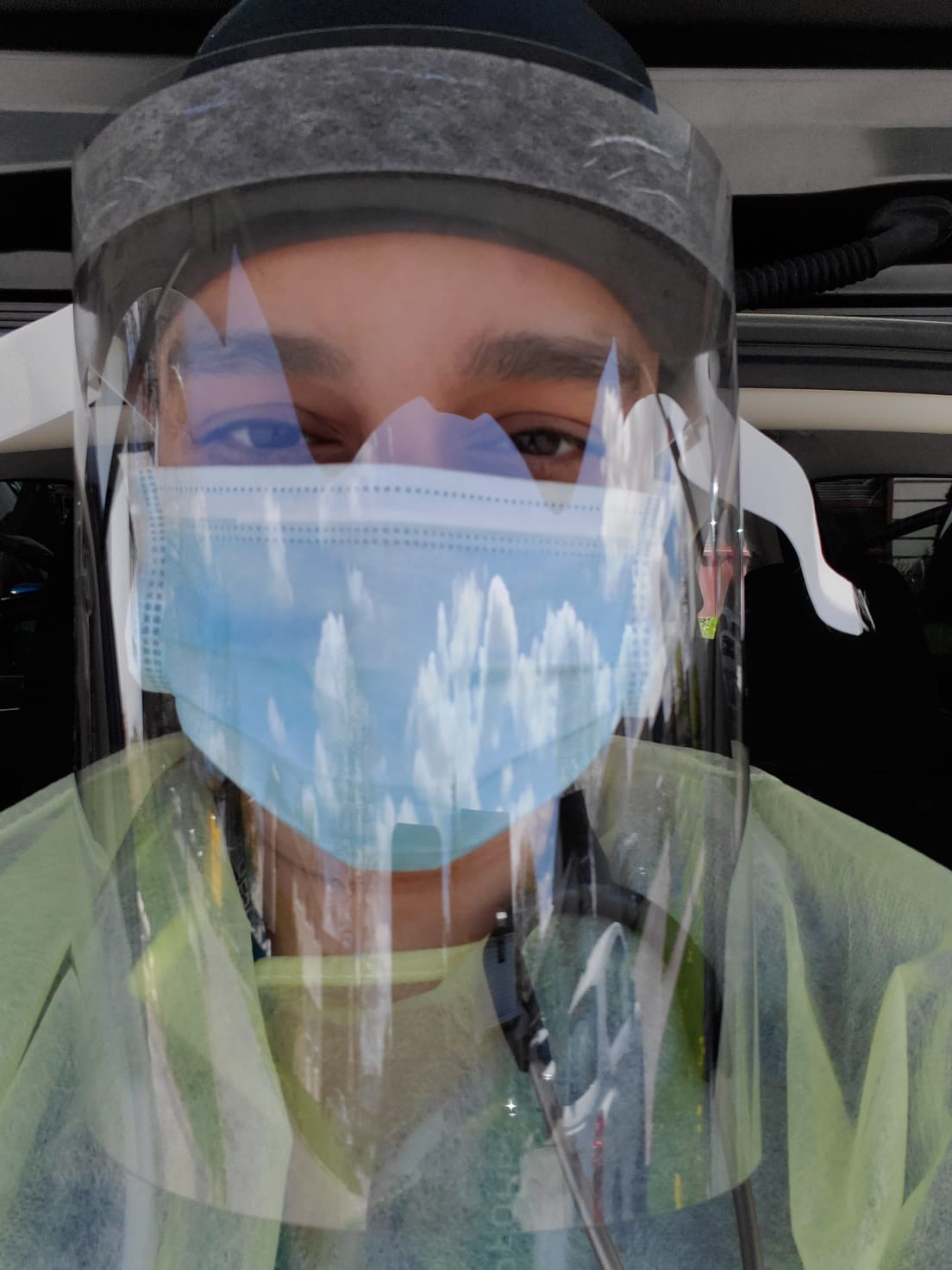
Navjit Kaur shares a selfie she took wearing PPE.
(Navjit Kaur)
That fear is something she couldn’t leave behind at the hospital.
“I was terrified and I did not want anyone in my family to have to go through what I saw in the hospital.”
Kaur spent weeks hidden in the basement of her home away from her preschool children during each wave of COVID.
“My husband and I decided that I would live in the basement until it was safe. But not being able to be with your family is very difficult.”
Her children could not understand why they were living apart, away from their mother.
These are the sorts of inhumane costs that society seldom considers, unbearable costs that many nurses no longer wish to endure.
Kaur avoids meeting her own parents.
“There's still a chance you can still catch something. Right? It was something I did not want to mentally take on, if I'm responsible for someone's death in the family.”
With patients streaming into Brampton's lone hospital, it was mentally devastating and frightening for staff.
There were days when burnt-out colleagues would get together to carry emotionally drowning workers to shore.
“When one of us was having a low day, we would pick her up, help push forward and keep going, on to the next patient and the next and the next.”
Away from her colleagues and family in her basement, there was no one to pick Kaur up.
“I would come home, I would be in tears breaking down because of everything I saw and then I would just get myself together again just so I could FaceTime or just kind of see [her kids] from the stairs.”
All of it, everything nurses have suffered through for almost two years, the ludicrous hours, lack of support from the provincial government and indifference from many administrators in the healthcare system, has been made almost impossible to bear due to one particularly alarming move by the Doug Ford PC government.
Dr. Doris Grinspun, the chief executive at Registered Nurses' Association of Ontario (RNAO) says nurses are walking away from the profession in droves and it’s the patients who will suffer in the end.
“The nurses cannot ethically and morally withstand what they are seeing.”
In an open letter to Premier Doug Ford, Grinspun called for the Ontario leader to repeal Bill 124, which was passed in 2019 and caps the increase to wages for most nurses at one percent during a “moderation” period to help the Province improve its financial situation.
Instead of being able to fairly compensate nurses who should be getting large salary increases for the herculean responsibility they have shouldered, the PC Bill disincentivizes nurses and public health workers whose wages have been capped with a one percent increase.
While employees in non-essential work take home large bonuses this holiday season, as many industries see record profits, nurses who have literally kept society running are being treated by the PCs with contempt, despite all they have done, say leaders who are trying to advocate on behalf of frontline healthcare workers.
Patients are still crammed into emergency rooms, sometimes for many days, and the shortage of staff as infection numbers steadily climb over recent weeks isn’t seen at just one hospital, Grinspun says.
During a Nov. 14 rally against the wage suppression law, Dr. Grinspun beseeched Premier Ford to repeal Bill 124 within 30 days. The time is running out for Ford and as of today there are now 2 days left to meet the stated deadline.
The RNAO and the Ontario Nurses Association have asked Ford and the PCs to exempt nurses from Bill 124, considering what the profession has gone through and the mass exodus of professionals from the field, but the requests have fallen on deaf ears.
The RNAO just launched a Twitter campaign, #StandWithNurses, calling all Ontario MPPs to tweet and demand Bill 124 be repealed.
As per Talkwalker, a social media analytics firm, the hashtag #StandWithNurses has currently reached about 1.7 million users.
“It is not the hospital's fault, right? It is the system; the Premier needs to understand that sooner or later he has to repeal that Bill,” Grinspun says. “There is no doubt in my mind about that.”
She says although there are some new nurses being brought on, the seasoned ones to mentor them are leaving.
According to the RNAO Nurses Wellbeing Survey, an increasingly high percentage of nurses, a majority of these 25 to 35 years old, indicated they were very likely (9.3 per cent) or likely (7.1 per cent) to leave nursing for a different profession after the pandemic.
“The veteran nurses are at an age that they can afford to retire, they're the ones walking out. So it's very, very difficult and the consequences on patients because patients cannot get the level of attention that they need,” Grinspun says.
Nurses, she adds, are unable to provide the care they can because they are stretched to the limit.
And while many senior nurses are calling it quits, the already stretched healthcare system does not have enough nurses to fill in the void.
“To bring international nurses up to Canadian standards takes years and cannot happen overnight, so at least give us something that is in your control,” Grinspun says.
Burnt-out nurses are out of oxygen and the Bill is choking them, she says.
“The only thing that is in complete control of the premier is Bill 124. The only thing is his complete control. And he could do it overnight.”
Ontario Nurses’ Association President Vicki McKenna, said, “While saying he ‘loves’ nurses, Premier Doug Ford has actually passed legislation to suppress their wages, override their collective agreements, give their employers unprecedented powers to redeploy them anywhere, deny vacation and more.”
Dr. Grinspun, who has worked in Canada since 1989, says the province is cultivating a system where people are afraid to talk.
“When people start to be afraid of talking, and that goes even for some presidents and CEOs of hospitals, that is serious, because then that person pushes down silence to the manager and eventually to the nurses.”
Some doctors did speak out and took a stand, but some were silenced.
“Dr. Brooks Fallis was fired, I was in the campaign standing up for him,” she says.
Dr. Fallis was the critical care interim head at Brampton Civic before William Osler removed him from the position after he spoke out against Ford government's pandemic response, he has said.
Osler has claimed the move not to consider Dr. Fallis for the job permanently had nothing to do with his criticism of the government. He was not given the opportunity to hold the job permanently, despite widespread support from the ICU doctors and other staff he worked with.
He was not the only one, another doctor was ostracized before he would end up resigning from the Ontario Science Table, Grinspun says.
“Dr. David Fisman, the country’s chief epidemiologist, left the science table because he kept saying COVID is airborne, we need a different type of protection for workers, for teachers, etc. but nobody listened,” she says.
Another doctor, Nathan Stall, was singled out and he has decided to run for the Liberals in next year’s provincial election, she says.
Kaur, the respiratory therapist at Brampton Civic, too has entered the world of politics to “fix the system”.
Kaur lost the federal elections to Kamal Khera in 2019, but is ready to contest Brampton West provincially, with the Ontario NDP.
She says putting a cap on nurses’ wages is disrespectful and amounts to telling nurses they are not important anymore.
“Nurses haven't been given that kind of respect and dignity that they deserve, after everything they've done, they are exhausted and you put a cap on their wages?”
Dr. Grinspun says while healthcare workers serve to protect patients they have this unsaid responsibility of protecting the system as well.
“We need to get hold of our system, because it's not the system of any particular politician, it is the health system of Ontarians. It's paid by taxpayers. Everybody has the same right to the health care system and that's what defines Ontario and Canada.”
“We want Bill 124 repealed and I would advise the premier to move ahead soon because the sad part is the nurses are not waiting. They're leaving every day,” Grinspun says.
“The premier needs to act like yesterday.”

Protests have been ongoing against Bill 124 and the provincial government's decision to cap wages for nurses.
(RNAO)
Nurses have faced mounting challenges since the start of the pandemic.
Cadet recalls there was a lack of personal protective equipment (PPE) when COVID-19 first began overwhelming healthcare settings, which began months of stress over the lack of support from government and administrators.
“There were not enough masks for the nurses and homecare was the last one that could receive PPE,” she says. “That period was very stressful because we were worried not to contract the COVID and to give it to clients or even our own family.”
Manuel says there were issues with emergency supplies that once required by a patient, must be delivered as soon as possible.
“When you need an arterial line insertion kit you kind of need one right then and there,” Manuel says, “So what nurses had to do is start cobbling together equipment to try and make one, which takes extra time, which is stressful.”
“That’s just an average day.”
If working twelve hours [often more] per day while fearing for your own life was not stressful enough, the pandemic had much more in store for nurses.
Death is always a part of the healthcare profession, especially in emergency departments, but the pandemic saw a new level of sorrow for nurses to contend with. They had to learn to deal with death on a scale many were not accustomed to. The trauma of losing a life in front of their eyes was now happening multiple times a day.
“We had four to five people die per shift, but you had to just move from that person to the next person,” Manuel says. “So if someone was dying, it was the nurses who were there with them in the last moments because families were not allowed in early pandemic months.”
The public needs to understand nurses have an innate ability to know when someone's in their final breath, Manuel says.
“We never leave people by themselves, we are always there to have a hand on the shoulder, to say, you've been in this life, you're moving to your next phase that you're not alone.”
Nurses will go as far as they can to save a life, but not every patient can win that fight.
“As a nurse we have to declare their time of death and that’s a solemn task, but it's also quite sacred,” she says.
For Kaur, these deaths brought on additional trauma.
Kaur’s grandmother had passed away from pneumonia and seeing elderly patients in COVID induced pneumonia took her back to her grandma’s last breaths.
Patient’s family members, especially from the Punjabi community, would run to Kaur for help.
“Those families come to you asking — will you please save my son? Can you save my grandma? Do you think they’ll make it next week?”
To deal with the continuous trauma that nurses go through, Manuel says, they have to seek out ways to practice therapeutic relationships with the patients they care for.
“Be empathetic, not their best friends,” Manuel writes in her blog.
She says as a registered nurse you can't be a friend to patients, and nurses have to set-up boundaries for these “therapeutic relationships.”
“You know the word, translucent? It's a bit murky, it's blurry, it's not completely clear, it allows you to see what's happening, but you don't have to be right in the middle of it to see it happening. Like you observe it, you watch it, but you don't have to feel it. That's part of the boundaries that we put up for therapeutic relationships.”
But this is not always easy to attain.
Manuel says when patients speak about their families or children, it can be difficult to not become emotionally involved emotionally while carrying out their work.
“We have to be able to disengage and tend to other grieving patients, when you have all kinds of other stressors happening, it becomes even more important to be present, but not lose yourself in the situation.”
When the pandemic was at its peak, Manuel was helping others fight burnout.
“You have to be a bit selfish, your family and friends have to step up and actually look after you so that you can go to work and do the work you need to do.”
Manuel says nurses spoke about neighbors coming together, leaving dinners at their doorstep with a short note or thank-you card.
“There was a lot of pot banging in the winter of 2020, that was just people finding some way to express their gratitude. Because what's interesting about nursing, it's rather invisible until you need it.”
The pandemic was not just a learning experience for nurses. Families had to learn to stay apart, in the same household.

As per a Nurses Wellbeing survey, families have played a major role in helping healthcare workers cope up with stress.
“My family knew not to hug me when I came into the house,” Manuel recalls.
Families play a big part when it comes to helping nurses cope with physical exhaustion and stress.
Manuel recalls there were a few occasions when her father would pour some scotch over ice for her, sit quietly and listen as she poured her heart out.
“Whatever had transpired that had caused me to come home and to be quiet, he respected that, but he also knew I needed to get it off my chest,” she says.
Many immigrant nurses that have more than one country to call home often find momentary joy, a temporary pain-killer of sorts in times of stress, in phone calls with their loved ones, but for Cadet, the COVID-19 pandemic stripped her of the little destresser she had.
She says she used to be on the phone with her family back home more often before the pandemic hit, but now finds it harder to keep in touch with them.
“The time difference is so hard, but I didn’t really have the energy left to call in to talk to family,” Cadet says.
The pandemic aggravated burnout in the profession that was simmering before COVID-19 arrived, the wage cap has only made things worse for a group of professionals who have been saving countless lives throughout the pandemic — without a break.
Manuel says nurses were not only working extra hours throughout the early stages of the pandemic, but were told they were not going to be taking any vacation in 2020.
“2021 came and now it's like — can we have vacation now? And it’s like we're going to limit who can take vacation and how much.”
To recuperate from all the mental commotion at work, Manuel has her own little prescription.
“I sit on a rock near water with a big sky above me, with trees moving in the wind, and that’s what I need, to sit there and listen to nothing — just breathe,” she says. “You can do everything right but someone can still die, and you can really muck up and somebody will live. It doesn't seem very fair at times. But it is what life is about.”
Manuel says Ontario needs a nursing task force like the Province had in the 90’s, which could help recruit and retain nurses.
Acute care nurses are paid, sometimes 40 to 50 percent more than community health nurses, Manuel says. Long-term care nurses also make less than those nurses who work inside Ontario hospitals.
“What they're trying to say is that the elite performers work generally in the hospital, which is really short-sighted because nursing is about excellence of care anywhere,” Manuel says.
For the 48-year-old Cadet, this difference in pay is the primary problem, which can prevent people from seeking out nursing positions in long-term care or homecare settings.
She says there is a huge difference between the payscale for hospital nurses and nurses in homecare.
“There is no consistency or equity, homecare is way behind compared to the hospital nurses.”
But the difference in pay is not the only problem.
“What makes matters worse is now people have more comorbidities than before, they live longer, but they have more health issues, which requires more care, more manpower,” Cadet says.
Another difference, Cadet says, between hospital and homecare nurses is often the work doesn’t stop at their client’s home.
“When you leave the hospital even though you're exhausted you are done [for the day], but with homecare, when you go home, there are the tasks that you still have to do,” she says. “We need to order supplies for the clients for the year, send letters to doctors and this is again after you go home exhausted, but you have to do these tasks to complete the client care.”
The thought of switching to long-term care or moving to a hospital does cross her mind.
“Some days it does make you think because you have to take care of yourself as well, but you stay for the future of homecare,” Cadet says.
Manuel says many nurses are losing their empathy because of mental, emotional exhaustion but they don’t want to admit it. Others are leaving the profession simply because they can no longer cope with the stress.
“There’s a critical care pediatric nurse that quit the profession, you don’t want to lose that knowledge and experience and it may have been that she needed time off to reevaluate life,” Manuel says.
“That’s the challenge there and that’s quite tragic.”
Email: [email protected]
Twitter: Anukul_AT
COVID-19 is impacting all Canadians. At a time when vital public information is needed by everyone, The Pointer has taken down our paywall on all stories relating to the pandemic and those of public interest to ensure every resident of Brampton and Mississauga has access to the facts. For those who are able, we encourage you to consider a subscription. This will help us report on important public interest issues the community needs to know about now more than ever. You can register for a 30-day free trial HERE. Thereafter, The Pointer will charge $10 a month and you can cancel any time right on the website. Thank you
Submit a correction about this story
