

New data show Ontario’s terrible approach to testing turned Peel into COVID hotspot
During the first wave of the COVID-19 pandemic it was impossible to escape public health messaging by local, provincial and federal officials.
The three practices hammered home by the hour were to socially distance (a minimum of two metres), wash hands regularly and, eventually, don a face mask whenever in contact with others.
The messaging wasn’t simplistic, it was important. Public attitudes and behaviours needed to be shaped to fight a deadly virus spreading rapidly into every corner of our planet.
But, in a display of hypocrisy, while these same officials told all of us how to behave, many either refused or at least willfully ignored much of the epidemiology and science of virology that medical experts began to share with them.
For the first few weeks there was not a clear understanding of testing and contact tracing, the two tools public health authorities could directly deploy to control viral spread, if governments cooperated.
In jurisdictions around the world where they did, the virus was effectively confronted, and in places like South Korea, a hyper focus on testing and tracing almost immediately eradicated the novel coronavirus.
In places like the U.S. it was an opposite story, and a country with about 4 percent of the world’s population quickly accounted for 20-25 percent of global COVID-19 cases.
Canada, was somewhere in the middle, and Ontario was somewhere in the middle of the country, in terms of testing and tracing levels per capita.
But in Peel, and Brampton specifically, it was another story entirely.
Premier Doug Ford and Health Minister Christine Elliott repeatedly claimed they were taking their cues from public health experts, but new data released by the Province show that viral literacy beyond distancing, masking and handwashing did not sink in with the two people who wield more power than anyone else in the fight of our lifetime.

Premier Doug Ford and Health Minister Christine Elliott
They were responsible for a strategy to guide Ontario through its COVID-19 storm and keep residents of Peel safe.
The key to any strategy was testing. "We've got to be able to test widely in the community for asymptomatic spreaders of the infection," Dr. Anthony Fauci, director of the U.S. National Institute for Allergy and Infectious Diseases, recently told the CBC, warning Canada was at a tipping point in its response to the virus. “If you just test people who are symptomatic, you're going to miss a very large contingent of the spread of infection in the community."
But in Brampton, from the beginning of the pandemic, both asymptomatic and symptomatic testing fell far short of any meaningful outcome. The testing levels were so low, they were effectively useless.
While Toronto was provided with 17 assessment centres and Mississauga received 3, Brampton, with a population of 650,000, was given 1, inside Peel Memorial, where between 150 and 300 tests were being done daily around the start of the pandemic.
There were no drive-through testing sites, unlike in other jurisdictions, such as Etobicoke, where the same healthcare system, William Osler, that runs Brampton’s hospitals, was resourced to run two screening sites, including one where residents could drive up in their cars and be tested without getting out.
In Brampton, at Osler’s lone screening facility, long lines became a feature immediately in the spring, and it was clear the city, because of certain employment and demographic patterns, was going to be a major problem.
But additional resources for testing in the city were ignored by the same leaders on TV every day telling us to distance, wear masks and wash our hands.

Long lines at Brampton's lone drive-through assessment centre became a fixture midway through the pandemic when the facility opened.
At its most basic level, testing allows officials and other experts to understand where the virus is spreading and where it is not. Testing data informs reopening policy, the protection of long-term care and acts as a trigger for lockdowns, as well as the signal for any loosening of restrictions.
No part of the viral response is easy. The virus that causes the COVID-19 disease is aggressively contagious, jumping from one person to another through close contact or in situations where airflow is limited. To compound the issue, an incubation period of up to two weeks means testing data offers a snapshot of the past and must be manipulated to understand the future.
In Ontario, new data released by the Province suggests efforts to expand testing since the first wave of the pandemic have focused on Ontario as a whole and not problem areas, particularly Peel. Analysis by The Pointer of several key moments between May and November reveals a rigid strategy that increased testing evenly across Ontario, instead of zeroing in on hotspots. Peel Region, where the virus is once more sweeping through already vulnerable communities, offers evidence of this.
Despite positivity rates consistently above (and regularly double) the provincial average, Peel has received marginally less testing than Ontario overall. Few targeted efforts have been made to proportionally increase tests in the region based on need and a constantly worsening pandemic in certain areas of the region (outside a brief period between late July and mid-August, Brampton has not seen any relief from high daily infection numbers since the end of March). Now, with a test positivity rate above 15 percent, and daily infections averaging almost 300 cases, Brampton has become the symbol of neglect.
To put into perspective the disconnect between the data and what officials did with it, consider these comments from mid-October.
“Three per cent is worrisome,” Ontario’s associate chief medical officer of health, Dr. Barbara Yaffe, said at the time, when the overall test positivity in the province reached 2.2 percent. Meanwhile, Brampton was approaching double digits, and public health officials, along with our political leaders including Ford and Elliott, knew it.
An analysis of the failure to use available data and create responsible testing capacity in Peel was done by The Pointer. It focuses on four key dates.
The first, in May, represents the highest point of the first wave outside of April, for which testing data is not available. The second, at the beginning of August, marks one of Ontario’s lowest infection periods and the day after Peel entered the most liberal restrictions since the start of the pandemic. A third date in late October was selected to coincide with the day Peel’s medical officer of health, Dr. Lawrence Loh, finally acknowledged a second wave had begun in the region, more than a month after his provincial and federal counterparts declared a second wave had arrived and two months after it had already hit Brampton. The final data point analyzes the most recently published figures.
Two key metrics are included in the analysis: the seven-day average of percent positivity and the seven-day average of tests per 100,000 residents. The percent positivity, or percentage of tests that show a person is infected, is used to measure if an area is testing enough, while tests per 100,000 offer the opportunity to compare screening levels between regions and across Ontario as a whole.
May
On May 24, Peel’s seven day average for percent positivity was 10.3 percent. By comparison, neighbouring Toronto recorded a test positivity of 8.9 percent. In Peel, 62 tests were administered per 100,000 residents, with 75 in Toronto. Overall, Ontario had a positivity rate of 5.3 percent and completed 61 tests per 100,000 across the province.
Despite double the rate of test positivity in Ontario, Peel was getting the same amount of testing done per capita.
It was the first sign that the hotspot was being ignored.
In May, the pandemic response was well underway, but Ontario was already on the backfoot. The government had mandated an emergency shutdown in March and was scrambling to protect hospitals, while losing its battle in long-term care. It was still grappling with a testing strategy: reacting to crisis points and failing to plan forward.
As restrictions played their part and cases began to fall, Ontario looked at reopening. In June, Peel Region entered Stage 2 of the Province’s old reopening framework and, by August 1, indoor dining, gyms and bars were all open under Stage 3. Over the summer, with lower rates of infection, leaders were provided with a golden opportunity to create a more responsive testing strategy than the one scraped together between February and June. There was a moment to breathe, evaluate and assess before the inevitable second wave, which epidemiologists around the world had made clear was on its way.
August
By August, the Ontario viral picture was vastly improved, although Peel rates (driven by daily case numbers in Brampton that were four to six times higher than Mississauga) remained well above the province’s overall.
On August 1, Peel’s positivity rate of one percent (brought down by Mississauga and Caledon) was double the Ontario figure of 0.5 percent. In Toronto it sat at 0.4 percent. Despite this, Peel recorded 124 tests per 100,000 residents compared to 158 in Toronto and 167 for Ontario as a whole. Peel’s rate represented a 100 percent increase over May, well below a 174 percent increase for Ontario as a whole. But instead of increasing testing in Peel, relative to screening levels across Ontario as a whole and compared to areas such as Toronto where screening capacity was expanded by a higher rate compared to its heavy hit neighbour to the west, screening here did not reflect the indicators that showed Peel was in trouble.
This pattern suggests a relatively inflexible testing strategy, ignoring historical and point in time test positivity rates. Instead of learning from Peel’s first wave and earmarking extra resources to keep the region under control, testing was increased across the board, despite data that clearly showed Peel was being hit much harder than other regions. In both May and August, Peel Region had a positivity rate twice that of the province as a whole, but was resourced for similar or lower testing levels than the average.
Using testing to get a general survey of the viral landscape is important, but zeroing in on specific problem areas is the key, according to epidemiologists. Identifying areas like Peel as a hotspot without creating more testing and contact tracing to control viral spread can be pointless.
“The best way to [increase testing] is to make sure that people in counties with high positivity rates have access to testing and are proactively getting tested when they need it,” Dr. Charissa Fotinos, Washington State’s COVID-19 testing leader, explained in September. “Right now, this is not happening enough, and we need it to drastically increase if we are going to stop COVID-19 from spreading rapidly, especially in disproportionately impacted communities and among our essential workers.”
By the summer, it was well known that demographics in parts of Peel, particularly in Mississauga’s Malton area and a number of neighbourhoods in Brampton, were more susceptible to viral spread, because of higher levels of employment in essential-work sectors such as food services and certain manufacturing industries, along with more dense living conditions and lower income levels which are correlated to factors such as a reliance on public transit.
But instead of using all these known indicators and the other data being provided, to increase testing levels dramatically, above any other part of the province, which should have been done, testing in Peel, particularly in Brampton, remained far below where it should have been to keep communities safe.
A high positivity rate tends to signal a lack of testing and an increase in tracked and untracked viral spread. In Ontario, including thresholds established by Peel Public Health, 2.5 to 3 percent test positivity indicates viral spread is not being controlled. New York City recently closed many of its public schools because the test positivity for the city as a whole reached 3 percent. At the same time, Brampton’s was over 15 percent.
Rates exceeding these benchmarks mean testing levels have fallen far short of the numbers needed to allow contact tracing to catch infections in the community before people transmit the virus widely out in public, allowing spread to take place relatively unchecked. Portable and flexible resources should be available to blitz these areas until the infection is brought under control. To recycle an overused metaphor: significant, portable testing resources would act as air support to dump water on the heart of a forest wildfire.
“A high percent positive means that more testing should probably be done—and it suggests that it is not a good time to relax restrictions aimed at reducing coronavirus transmission,” David Dowdy and Gypsyamber D’Souza from the Johns Hopkins Bloomberg School of Public Health explained in an August article on test positivity.
Between August 1, when a semblance of normality returned, and October 26, when Loh finally proclaimed a second wave in Peel, the COVID-19 picture went from decent to dire.

Dr. Lawrence Loh, Peel's medical officer of health
October
In less than three months, Peel’s positivity rate jumped to 7.1 percent on October 26, far outpacing either Peel Public Health or the Ontario targets for keeping the virus under control. Tests did increase to 181 per 100,000, an uptick of 45 percent. But by comparison, Toronto, with a test positivity of 4.6 percent, completed 214 tests per 100,000 on the same day near the end of October, an increase of 35 percent from its August levels. Ontario as a whole (with a test positivity of 2.9 percent at the time) increased its average 25 percent to 210 tests per 100,000. Both Toronto and Ontario remained well above Peel’s testing per capita, despite the region’s dangerous positivity rate, which was three times higher than the rest of the province.
Despite Ford calling Brampton “broken” on September 4 and Elliott repeatedly claiming the city would get more testing if it needed it, both of them ignored their own responsibility, and the data that was staring them in the face.
In early November, Loh demonstrated an understanding of the importance of ramping up testing for areas with high positivity. “Either we’re not testing [enough] or we’re seeing … a true rise in cases, or both,” he said on November 4 to Mississauga councillors, with Peel’s positivity rate already twice as high as the next worst part of the province. “Until we actually finally get a little more data, especially with our testing levels continuing to be brought up, we’re going to have to just assume that it’s both. We’re not testing enough and we’re seeing a genuine rise in cases.” What he did not explain, was that the “genuine” rise of cases was largely due to inadequate testing and the crucial contact tracing that can only be done effectively with proper testing levels to show tracers where to look for viral spread.
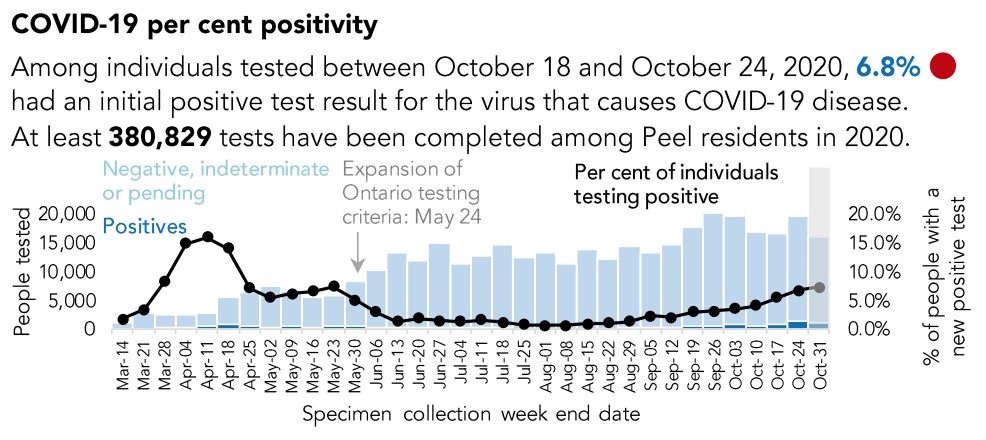
Test positivity data in October, which showed 6.8 percent of COVID tests in Peel were coming back positive, indicated an increasingly dire viral picture for the region.
Other officials, particularly Elliott, have shown a lack of understanding of the dire reality in Peel. On September 14, The Pointer asked her why Brampton had operated with just one full testing centre for the entire pandemic (Osler has since opened its Cold and Flu Clinic at Memorial providing another option for residents wishing to get tested) and how she would improve the situation.
“If we find that there is a need for another testing centre in Brampton, of course, we will take a look at that, because we want people to go and get tested and distance from the testing facility shouldn’t be a problem that hinders them from doing that,” she said. Provincial data for the day she spoke show Peel Region had a test positivity rate of 2.1 percent compared to a provincial rate of 0.9 percent, and, using population per municipality, Brampton’s would have likely been closer to 4 percent. In Brampton, Mississauga and Caledon, 155 people were tested for every 100,000 residents, 22 percent below the provincial rate of 199, despite Peel having more than double the test positivity rate compared to Ontario overall.
It seemed incomprehensible that Elliott would not have known Brampton desperately needed much more testing.
After promising to look into the issue, and in the face of her own data, nothing changed.
At an October 28 press conference, The Pointer again asked Elliott about Brampton’s testing resources as the city continued its status as Ontario’s hotspot. "We will look into what is happening in Brampton,” Elliott said.
When she spoke, 44 days after she had last offered a similar answer, the picture in Peel had worsened significantly. The region’s positivity rate had increased 238 percent to 7.1 percent (Brampton’s rate was likely above 9 percent). Ontario had a rate of 2.9 percent. Testing in Peel had increased 15 percent to 178 tests per 100,000 residents. Still, Ontario as a whole was tested more thoroughly, with 208 tests per 100,000.
Elliott’s carbon copy answers, twinned with Peel’s skyrocketing positivity rate, illustrate a rigid approach to testing. The data portrays a paralyzed government unable to move and adapt to a rapidly spreading virus. While Brampton recorded as many as six times more daily cases of infection over long periods between August and late October compared to Mississauga, it maintained three official assessment centres as Brampton suffered with just one lone testing facility.
For a community as diverse as Peel, with significant visible minority populations and thousands of essential workers, this rigidity is punishing. “When scarcity does not permit mass testing, equitable allocation needs to take into consideration the risk of infection and from infection, including risks to economic well being,” University of Michigan experts Ryan Huerto, Susan Dorr Goold and Duane Newton wrote in June. “Those most at risk for worse health outcomes, and those with precarious financial stability, need to be prioritized.”
In Peel, these considerations have not been taken into account.
Recycling one more military analogy helps to drive this reality home. In a battle with the virus, Peel is Ontario’s weakest line of defence; it is the front the province is most vulnerable on. Without new munitions, reinforcements and a targeted game plan to shore up ranks, the virus will continue to break through the region and spread elsewhere.
November
On November 9, Peel’s positivity rate sat at 10.6 percent, Toronto was at 5.8 percent and Ontario at 3.9. Yet, as has been the story of the pandemic so far, Peel was only able to test 194 residents per 100,000, compared to 217 in Toronto and 211 across Ontario.
The failure to properly resource Peel, and Brampton in particular, has been one of the great tragedies of this deadly pandemic, and the Province’s own data proves it.
Email: [email protected]
Twitter: @isaaccallan
Tel: 647 561-4879
COVID-19 is impacting all Canadians. At a time when vital public information is needed by everyone, The Pointer has taken down our paywall on all stories relating to the pandemic and those of public interest to ensure every resident of Brampton and Mississauga has access to the facts. For those who are able, we encourage you to consider a subscription. This will help us report on important public interest issues the community needs to know about now more than ever. You can register for a 30-day free trial HERE. Thereafter, The Pointer will charge $10 a month and you can cancel any time right on the website. Thank you.
Submit a correction about this story
