

‘Anything is better than this’ – a doctor describes the pain of Peel’s sickest COVID-19 patients
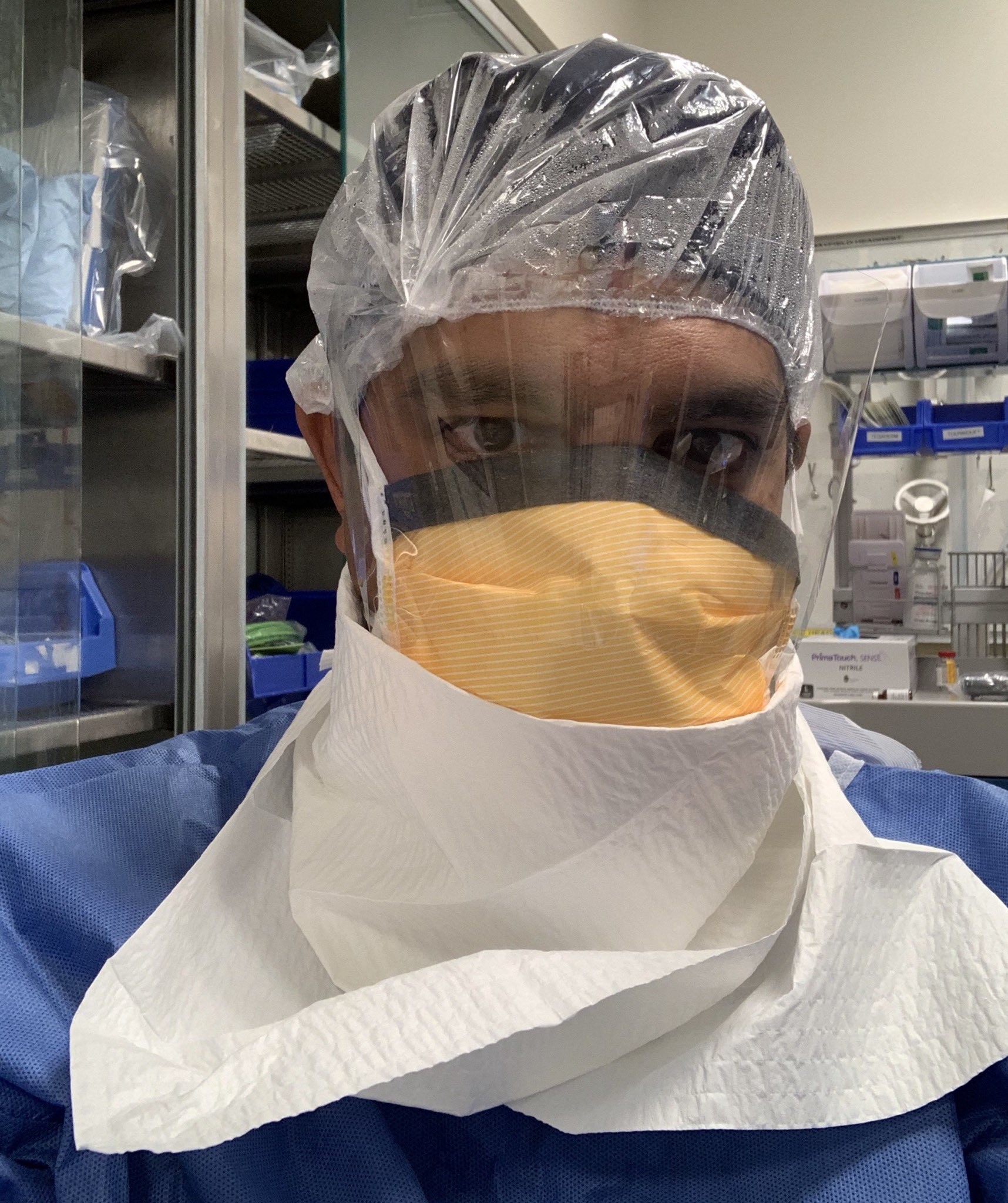
If you’re in a battle against COVID-19 at Mississauga Hospital, the masked face of Dr. Rohit Kumar is a blessing, a sign your laboured breathing and choked coughs may finally get some help.
It can also be ominous – his face may be the last you will ever see.
As a veteran anesthesiologist, Dr. Kumar is part of a team caring for the sickest COVID-19 patients at the hospital, sedating them, and placing them on a ventilator.
Mechanical ventilation is a last resort in the battle against COVID-19. Many who are placed on a ventilator never wake up.
“When we’re intubating someone we’re often the last person that that person is going to see before they potentially pass away,” Dr. Kumar says. “That’s a very real feeling.”
Dr. Rohit Kumar
According to numbers from New York City, the epicentre of the outbreak in the United States, 80 percent of patients placed on ventilators didn’t survive. It’s a statistic the doctor doesn’t want his patients thinking about when he’s putting them under.
“You’re so focused on doing what you can to make that patient better, everything else sort of falls by the wayside. Our job is complicated on many different levels and part of it in that moment is we really have to display a sense of confidence to the patient, who is basically struggling to hang on for their life,” he tells The Pointer. “They need to know that nobody is second-guessing themselves and they’re going to be well taken care of and to provide that reassurance is very important.”
Many who require ventilation have underlying conditions, like heart disease or diabetes or respiratory problems, and are typically seniors. Early in the pandemic, many in the younger population felt they had a free pass, partly because of the early numbers out of China that showed the elderly were being disproportionately impacted. A headache, perhaps a cough and fever, but nothing uncommon in the annual flu season, many millennials and Gen-Xers thought.
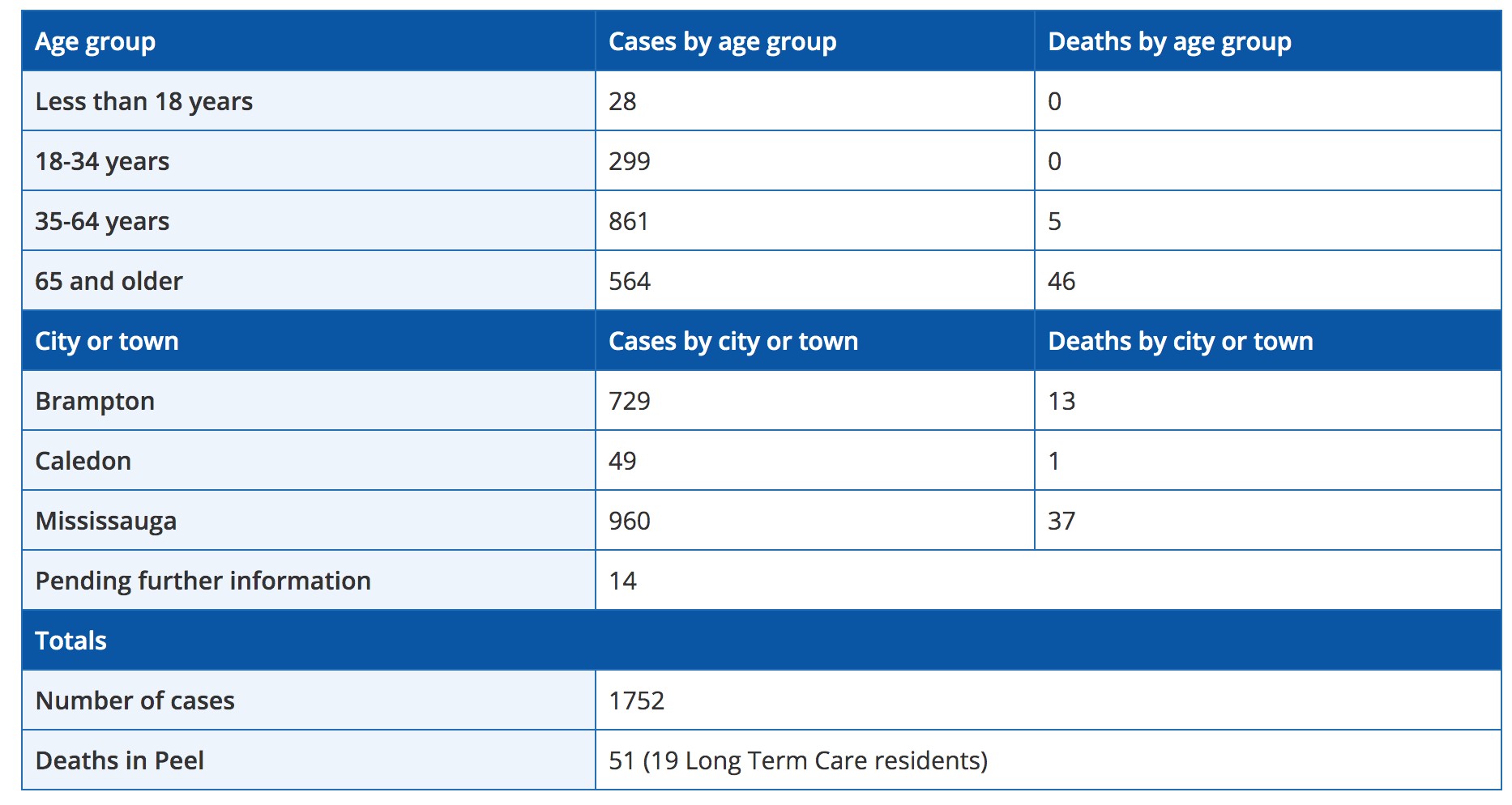
A breakdown of Peel's COVID-19 cases (as of April 21) shows the virus is particularly fatal in those over the age of 65.
It’s become clear this new virus is a bigger beast. The rapid spread across the country in a toxic burst of infection, and numbers that show this killer does not discriminate based on age, has even the young among us concerned.
“It’s a tough thing. We’re seeing young people too,” Dr. Kumar says. “I intubated a young person last week and they’re not doing well. They’re COVID-positive and we go in there, into their room, and we’re exposed to that, and then you think, ‘that could be me.’”
“The risk is real for us,” he says.
In the battle against the disease, the frontline has shifted several times since the first cases began to pop up in Canada earlier this year. First, the fight was in the air. Governments scrambled to put in place travel restrictions and screening protocols for travellers returning from recharging March break vacations around the globe. Then attention turned to the hospitals. As news from China, Italy and Spain began to filter home, the horror stories of overflowing emergency departments and ICUs, doctors faced with the paralyzing choice of who gets a ventilator and who doesn’t, spooked officials here. They scrambled to build capacity – no one, ever, wants to make a decision like that.
The effort, like those massive ones during war-time, which many only know about through books and documentaries, have been largely successful, as numbers show Ontario’s hospital system and its intensive care units are mounting a defence to protect our most vulnerable patients as the enemy looms.
Now, the front has shifted to long-term care homes and other densely populated institutions (shelters, group homes, correctional facilities) as the impact of the virus, if it slips inside these doors, would surely be devastating.
The proof is shown nightly on the news.
In Peel, there are approximately 20 long-term care homes dealing with ongoing outbreaks and 16 residents have already lost their lives.
For long-term care facilities and other seniors’ residences, COVID-19 can spread quicker than a bush fire, with the same deadly consequences. The bodies of those with pre-existing medical conditions, many at an advanced age, with shaky immune systems, exposes these vulnerable citizens to serious illness.
SARS-CoV-2, this predatory virus, does not make calculations before it kills. In Peel, it has struck people of all ages, and those 18 to 34 represent 17 percent of confirmed cases. Another 54 percent are between 35 and 64, and those over 65, surprisingly, represent only 27 percent of the region’s infected population.
In Ontario, the numbers are even more spread out, with each age bracket accounting for just over 20 percent of confirmed cases, except for those 40 to 59, who account for 31 percent.
While younger populations can still fall seriously ill from COVID-19, data shows it’s particularly fatal in the elderly. Of 32 deceased in Peel, as of April 16, 27 were over 65. The others were 35 to 64.
At the Trillium Health Network, which operates Mississauga Hospital and Credit Valley, the number of COVID-19 patients is rising steadily. As of Tuesday, the network was treating 96 COVID-positive patients, 26 of them in intensive care.

The front line of the battle against COVID-19 has shifted several times since the pandemic began, but so far, Ontario's hospitals have managed to deal with the increased pressure created by COVID-positive patients.
It’s unknown how many are on ventilators, but it’s clear that Dr. Kumar and his team are busy.
The virus is a Frankenstein monster of pathogens. It came to life in a Chinese “wet market” where all sorts of wild animals are bought, sold and butchered in close quarters, this mixing of animals, blood, feces and other organic matter, is thought to have created the virus – which eventually jumped from animals to humans.
The science of how COVID-19 first enters, and then attacks the body, reads like a horror story.
Droplets are expelled by an infected person when they cough, sneeze or possibly even when they talk and breathe, and can enter the body of a healthy person in different ways. A lot remains unknown about it, but it tends to prefer entering through the nose, binding to a particular type of enzyme called ACE2, which normally helps regulate blood pressure. Once inside, the virus takes over these enzymes and begins to multiply, which leads to the identifiable symptoms similar to the seasonal flu: fever, dry cough, chills, and a loss of smell.
For the more severe cases, like those seen by Dr. Kumar and his staff, the novel coronavirus invades into the lungs, entering the “respiratory tree”, wreaking havoc on our breathing organ.
The immune system responds, secreting fluids that fill the passages as the body’s own defensive inflammation makes it harder to draw a full breath. This is when a patient may need oxygen delivered by nasal prongs. But if the infection sets in further, finding its way into the alveoli (small sacs at the end of the respiratory passageways which help pass oxygen into the bloodstream and out to the rest of the body) things can go downhill quickly.
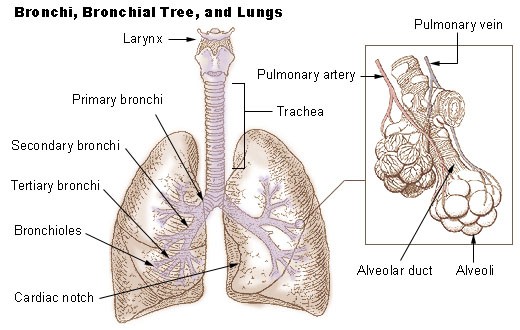
COVID-19 attacks the lungs in particular, as the body fights back, the small sacs (alveoli) which help carry oxygen to the bloodstream, can become clogged with fluid and pus, making it difficult to breathe.
The body’s immune response kicks in further to fight the infection, which can lead to a build-up of more fluid (pus) in the lungs – further clogging the airways and preventing desperately needed oxygen from reaching the body.
This dangerous dance is similar to pneumonia, something particularly deadly for the elderly. The key difference with COVID-19 is that the pneumonia it causes is not bacterial, and can’t be treated with antibiotics. The body must fight off the virus mostly on its own, and for the elderly and those with underlying conditions before contracting it, their immune-response will be weaker.
A ventilator takes over a person’s breathing, ensuring enough oxygen is reaching the body so it can continue to fight and keep all the organs from shutting down. If the blood is not properly oxygenated the body can go into shock and organ failure can begin.

Mechanical ventilation is risky, but necessary to keep someone alive so their body can continue to fight COVID-19.
Ventilation is a procedure fraught with risk at the best of times, and particularly dangerous for the care providers.
“That is probably one of the highest risk procedures that can be done because it puts you at a really high exposure risk to COVID-19,” Dr. Kumar says.
When the call goes out for a patient having difficulty breathing, he is one of a four-person team which rushes in to assist.
After donning all of the proper personal protective equipment (PPE), the first step is putting the patient under.
“We actually paralyze them so they won’t cough and aerosolize the virus, and then once they’re sedated, or put to sleep or paralyzed, we place the breathing tube in,” he explains.
The breathing tube is inserted down the person’s throat and once the other end is hooked to the ventilation machine (depending on the person’s medical state), it either assists or fully takes over the breathing process for their body.
At the start, the lungs are flooded with waves of oxygen — much more than the typical 21 percent oxygen levels we breathe from the atmosphere.
Throughout the majority of the ventilation process, the patient is kept asleep and delivered medications and drugs to keep them asleep through an IV.
“This gives the body a chance to rest and hopefully fight the infection, and then any supportive measures – whether it be fluids, or blood pressure medication – we can do that in a very controlled way to help support the patient,” Dr. Kumar says.
Throughout this process, doctors monitor the build-up in the lungs. The body’s automatic immune reaction to fight back leaves behind pus and other fluids that can impact the lungs. In a normal situation, a person is able to cough up this fluid on their own. For someone on a ventilator, a catheter tube, like a small vacuum, is inserted into the breathing tube and down into the lungs where it can suck up the excess fluid.
It can be a difficult procedure, one that has not been met with a lot of success for many COVID patients. But Dr. Kumar says most are more than willing to accept any help to make the pain go away.
“They’ll accept any risk because they just feel so terrible. They feel like they’re dying because they can’t breathe. At that point, in their minds, they’re probably saying, ‘I’ll accept anything – anything is better than this,” he says.
As of Monday, there were 193 COVID-19 patients on ventilators in Ontario hospitals.
There is no set time for keeping a person on ventilation. But, if they begin to show signs of improvement, they can be taken off the machine to breathe on their own.
It’s the first time the patient needs to be awake during the procedure.
“You can imagine, if you’re wide awake with that breathing tube in your mouth, it’s not going to be the most comfortable thing. So whether you’re a COVID patient or not, anybody who has a breathing tube in, when that breathing tube comes out, there is coughing and stuff that happens at that time,” Dr. Kumar explains.
This is the most infectious time during intubation. When the COVID-patient coughs, they are releasing infectious bursts of the virus into the room. The only thing between the doctors and the patient on the hospital bed, is multiple layers of personal protective equipment donned before entering the room. It’s hard not to worry in those situations.
“Obviously, this is a really bad virus, it’s claimed a lot of lives and continues to claim a lot of lives,” Dr. Kumar says. “From that standpoint, it is scary, and I think along the frontline there is a lot of fear of ‘what if you get infected, what if you take it home to your family and your kids?’”
“We have the equipment that is supposed to keep us safe, and we’ve practiced and we’re following the principles of safe care as best we can, and hopefully that will get us through,” he adds.
For Dr. Kumar and his wife — who also works in healthcare currently treating COVID-19 patients, they’ve implemented procedures when they get home to keep their children safe. They leave all their work clothes in the garage, and shower before they do anything else.
“From a family standpoint we’re taking extra precautions because we’re worried not just for ourselves, but we’re worried for our kids and our extended family. For sure, it definitely weighs heavy on the mind.”
In addition to those worries, doctors, nurses and other frontline professionals have had to deal with other concerns that have permeated throughout Ontario’s healthcare system during the pandemic.
First, were concerns around hospital and ICU capacity, then supplies of PPE which, for Dr. Kumar and his team is vitally important. He admits there’s been anxiety around the potential lack of PPE, but says Trillium has done a good job of preparing and gathering supply.

The potential shortage of personal protective equipment for frontline healthcare workers has been a concern throughout the COVID-19 pandemic.
The potential lack of PPE raises a lot of difficult questions for healthcare providers, whose first instinct is to help, regardless of the circumstances. “It puts us as healthcare workers in a very difficult position. When you see somebody who is not doing well, if you don’t have the equipment and they’re dying in front of you, it’s a very difficult thing not to go and help that person.”
In his 13 years with Trillium, the doctor has never seen anything like this virus, and it’s put a serious strain on everyone working the frontlines. But he says there are signs of hope.
“Even though people are burnt out and tired, I think the medical profession is a bit unique in that when it comes time for people to come together and get the job done…people have really united to tackle this,” he says.
“That’s a really amazing thing.”
Email: [email protected]
Twitter: @JoeljWittnebel
COVID-19 is impacting all Canadians. At a time when vital public information is needed by everyone, The Pointer has taken down our paywall on all stories relating to the pandemic to ensure every resident of Brampton and Mississauga has access to the facts. For those who are able, we encourage you to consider a subscription. This will help us report on important public interest issues the community needs to know about now more than ever. You can register for a 30-day free trial HERE. Thereafter, The Pointer will charge $10 a month and you can cancel any time right on the website. Thank you.
Submit a correction about this story
