

Is India the world's next COVID-19 ticking time bomb?
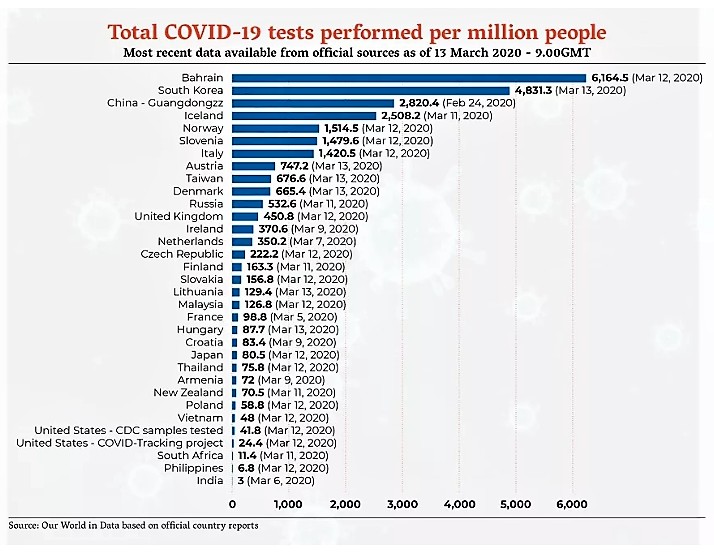
By March 13, India, a country of almost 1.4 billion people, had tested just three of them per every million for COVID-19. South Korea had tested 4,800 residents per every million by the same date.
It was becoming clear to medical officials and epidemiologists in the world’s second largest country that a problem could be spreading in their midst, a very, very serious problem. But they had no way of knowing how bad the threat of COVID-19 was in a country whose 800 million citizens in its underclass remain marginalized under a system of caste and have very poor access to healthcare.
If the novel coronavirus found a foothold in a country the size of India, where the majority live in or around poverty, with a lack of infrastructure and a healthcare system most have difficulty accessing, the impact could be profoundly devastating.

Screen grabs posted on Twitter show thousands of Indian workers Friday trying to travel home from a Delhi bus station
“As you test more, you’ll find more, which is exactly what you want to do,” says Dr. Prabhat Jha, an epidemiologist and founder of the Centre for Global Health Research at St. Michael’s Hospital in Toronto. “And when you find more you can then take the necessary steps to curb the growth of infection.
“Otherwise you won’t know how bad it could get.”

Toronto epidemiologist Dr. Prabhat Jha
In India, experts fear it could get incredibly bad.
“We expect 55 percent of the Indian people will get COVID-19 infection: 300 to 500 million cases over the next four months,” Dr. SP Kalantri, the medical superintendent of Kasturba Hospital in the central state of Maharashtra, told the U.S. publication Vox recently. “If the current disease trajectory is anything to go by, we expect 1 million or 2 million deaths in India over a one-year period.”
Dr. Kalantri received his Master’s in Public Health, specializing in epidemiology, from the University of California, Berkeley and collaborates closely with researchers at McGill University in Montreal, studying the spread of diseases.
“In Maharashtra, a state where I live, 60 million of 120 million are likely to get infected in a year,” he said.
Those frightening comments came before India stepped up efforts, launching a mass COVID-19 testing initiative and completely locking down the country this week.
Indian Prime Minister Narendra Modi made headlines around the globe when he announced the extreme measures, with police and military personnel now enforcing the severe restriction on mobility across the country’s suddenly deserted public spaces.
Having grounded all international flights in and out of the country to prevent the spread of COVID-19, Modi announced on March 24 an immediate 21-day lockdown of the world’s second most populous nation.

The country's lockdown has left the famed India Gate area in New Delhi empty
An estimated 1.4 billion people are not allowed to leave their homes, and could face significant reprisals for doing so, as was seen in the past week from widely shared footage of police armed with batons beating vegetable sellers and rural villagers, in some instances forcing them to take part in humiliating group calisthenics, as punishment for disobeying the national order to stay home.
The crackdown also ensnared thousands of visitors to the country. Among that number are at least 21,000 Canadians, who are now stranded in India and unable to leave the country, including Brampton and Mississauga residents whose family The Pointer has spoken with here in Peel.
India’s official reported figure — 887 confirmed COVID-19 cases as of Friday — doesn’t capture the reality, experts there say.
A lack of testing up until recently, has created an innacurate picture.
According to data released by the Ministry of Health and Family Welfare which is tracking case counts, India’s first reported COVID-19 case was discovered in the state of Kerala on Jan. 30.
Aside from some spikes, as well as a gap of nearly a month without any official count between early February and March, the numbers didn’t seem to be all that worrisome. But it was clear by the action India’s government was readying to take, that things were much worse. Hospitals were already reporting patients, who likely had never been tested for COVID-19, showing symptoms that were getting worse by the day.
When Modi announced the lockdown, the official count for the country was only about 300 cases.
But what isn’t being reflected in the data is how little testing for COVID-19 India has undertaken, which throws any official count into doubt. As a recent report from the Associated Press found, Indian health authorities were up until recently only conducting around 90 COVID-19 tests per day, well below capacity, leading to unreliably low numbers for infection. For context, South Korea, a country with less than four percent of India’s population, was testing almost 20,000 people a day earlier this month, to control the spread of COVID-19.
With such little testing across India, there is a very real concern the actual number of cases is far higher and the virus is spreading through the populace via community transmission.

“By not doing tests we may be under reporting or missing out on cases,” said former Indian health minister Kanuru Sujatha Rao in a recent interview with the Indian publication Caravan. She warned of the inadequacy of the current government’s response to COVID-19.
Dr. Jha thinks India would do well to look at the approach taken by countries such as South Korea, which offers a far more accurate assessment of the spread of infection.
Modelling of the actual rate of infection suggests numbers far higher than what’s being officially reported, and the makings of a national disaster.
If 35 percent of India’s population, close to 500 million people, are eventually infected (a rate not out of line with the rate being projected in the U.S., where some researchers predict a hundred million infections) medical experts there say the vast majority of these cases will be minor, but even a small percentage requiring hospitalization could eventually overwhelm India’s overburdened government-run healthcare systems. Hospitals in the publicly funded system don’t offer even close to the standard of care at India’s numerous private hospitals, which cater to the wealthy (including many foreign patients who flock to the country every year for treatment in its rapidly expanding medical tourism sector) and are considered among the best in the world.
Should infections rise exponentially like they have in the U.S., which as of Friday had passed the 100,000 mark for confirmed cases of novel coronavirus, the impact for India would be catastrophic.
As Kalantri stated, a worst case scenario could see as many as two million dead in a year.
Unlike other countries, such as Italy, whose healthcare systems are being overrun by the virus, India isn’t there yet. But the country is running out of time. There are promising steps being taken by the Modi government of late, expanding testing and engaging in more random sampling of the population to pinpoint possible infection clusters, but more needs to be done.
“Though these efforts are commendable, India needs to ramp up its efforts and respond more aggressively,” wrote public health researchers Manjunath Shankar and Anant Bhan in a recent editorial for the Indian publication The Print.
According to health experts, India must have a multi-pronged approach in its battle against COVID-19.
The first step is quickly scaling up testing. That’s already been aided by the government relenting and allowing private medical labs to take part in the stepped-up testing effort, but precious weeks where more local data could have been obtained have already been lost, Jha fears.
In comparison to India, South Korea aggressively tested for the virus and engaged in contact tracing, tracking the movement of known infected persons to determine where infection could have spread.
Along with an enhanced testing strategy, Jha says there needs to be “a big industrial push” for the production or purchase of enough supplies of personal protective equipment for healthcare workers: surgical masks and gloves to insulate them as best as possible from infection.
India also needs to rapidly increase its supply of ventilators required to keep critically ill patients alive.
There are no official numbers for how many ventilators are in supply, but a recent study by the Brookings Institute estimates that even under the best case scenario, where every hospital bed is fully equipped, there are only 57,000 ventilators for the entire country which can be dedicated for COVID-19 patients. If Kalantri is right, that as many as 500 million across India could be infected in a year, if even one percent require a ventilator, that would be five million patients, or approximately 416,000 a month, leaving the country, like many others around the world, woefully short of ventilators.
But unlike, for example, Canada, where a few thousand extra ventilators could dramatically help, India would need hundreds of thousands. How that many could be acquired remains unclear.
In addition to more equipment, Jha believes hospitals should be separated into two fully distinct wings with healthcare teams dedicated only to one section. Incoming patients must be rigorously screened so that if they do have the virus they are immediately isolated from non-COVID patients.
“Imagine the chaos if one infected person is in a hospital waiting room where there’s 300 people,” said Jha. “That one person could infect dozens.”
In the case of Italy, transmission was in part spread unwittingly by infected hospital nurses and doctors, showing no symptoms, to fellow healthcare workers.
A March 19 study by the International Council of Nurses found the virus by that point had spread to an estimated nine percent of all healthcare professionals in Italy.
“The high rate of infections among nurses and other healthcare staff is a serious concern because workers who are infected must stay away from work for at least 14 days, depleting the already exhausted workforce,” said the group in a press release.
If India’s already overburdened government healthcare system eventually sees similar statistics, it would be crippled, like the system in northern Italy.
India’s reporting of COVID-19 cases should have far more details, says Jha. National counts are unreliable and the total number of cases don’t line up with individual counts from states. There is no country standard for reporting, and there seems to be no impetus to standardize reporting across localities, critics in India have stated.

The Indian government introduced drastic measures this week to shutdown the country as testing for COVID-19 ramps up
Singapore on the other hand provides a much better picture for healthcare workers to track cases: ages of patients, when and where they were infected and diagnosed, where they traveled and who, or what, they may have contacted when they were infected. With that information, there is greater ability to build a better epidemiological understanding of the virus and use that for containment strategies. It can also create more public support for government health recommendations for COVID-19 like the need for physical distancing.
India’s Office of the General Registrar, responsible for compiling the national Census, also used to track causes of death in various areas through random sampling, but the practice was suspended in 2013, and Jha believes it should be immediately resumed, so as to better account for the number of deaths caused by the novel coronavirus, officially at 19 according to the government as of Friday. This total, according to some Indian medical professionals, fails to capture those occurring outside of a medical setting and those who might have died after contracting COVID-19, without it ever being diagnosed.
More reliable data coming from a municipal level, posted on a website and shared publicly would help locate previously unknown clusters, said Jha.
“So, If there’s a big spike in deaths that aren’t typical for the season, then you will know this is COVID-19, there’s a possible explanation,” he says.
Modi faces another problem: a lack of trust among many he has alienated. There have been several uprisings since the summer over a controversial citizenship Act Modi pushed, which curtails the rights of millions of Muslims. Mass protests over the new law were marred by religiously-fuelled violence in a number of states.
Social media footage in the last 24 hours captured Muslim worshipers coming out of Mosques in India, beaten by police for ignoring the lockdown.

It’s not an ideal political climate for the control of a killer virus.
Adding to divided animosities which have flared up between Hindus and Muslims over various points in the nation’s history is a compelling reason for some to disobey the quarantine measures: abject poverty.

Extreme poverty is widespread across India
Even with major economic growth over the last two decades, lifting the fortunes of millions of Indians, 5.5 percent of the population or 73 million people according to recent estimates, live in extreme poverty, making less than the World Bank’s international poverty line of $1.90 (USD) per day. Another 700 million live in what is considered to be the lower class, under India’s oppressive social caste system.
Millions live in very dense, tight quarters inside India’s teeming cities, which contain vast neighbourhoods without proper sanitary infrastructure and where electricity is often unavailable. Refrigeration to store food is not an option for hundreds of millions of Indians.

Tens of millions of Indians live in conditions that make it difficult to control the spread of disease
In an effort to ensure compliance with the 21-day quarantine, the Indian government unveiled a $23-billion (USD) aid package on March 26 meant for the country’s poor as well as allotments of wheat and rice it hopes will help feed some 800 million Indians for the next three months.
“We’ve immediately responded within 36 hours of the lockdown, said India’s Finance Minister Nirmala Sitharaman. “We’ve first reached out to the poorest of the poor, who need help.”
For the lockdown to prove effective, aid will need to be enough to warrant staying indoors, said Jha.
“It’s a really simple thing for the Indian government to organize for disaster relief, and then there’s an incentive for people to get tested and stay home,” he said.
Email: [email protected]
Twitter: @RG_Reporter
Submit a correction about this story
