

Brampton physician leading campaign for doctors who want no part in medically assisted death
Canada has an aging population which is growing at unprecedented levels. Incredible advances in modern medicine and extended peacetime are among the factors which have significantly increased average life expectancy. Cities such as Brampton provide the perfect example of just how unprepared Canada is for its senior population’s continued growth.
“We have a growing and aging senior population, which is predicted to explode over the next few years, and governments don’t have a plan for it,” Brampton physician Kulvinder Gill told The Pointer. “They don’t have the funding or facilities to cope.”
There’s a moral question, though, at the epicentre of the debate: when end of life care is strained, when should we choose to die?
Some doctors want to play no part in the process, except to try and preserve life.
“The Alberta model is acclaimed not only nationally, but internationally - they have a phenomenal model. ” Gill said. “They have a model where patients can call and are connected with a MAiD [Medical Assistance in Dying] team which consists of physicians, nurses and social workers; that team then goes to wherever that patient may be… they assess the patient where they are and then they connect them to someone to carry out their wish.”

Brampton physician Kulvinder Gill
In Ontario, physicians such as Gill have been lobbying to adopt the Alberta model for assisted dying. The argument is to allow the physicians who don’t believe in a certain procedure to focus on other things, while directing patients toward those who are comfortable with the process.
The history of doctors’ freedom of conscience dates back to the end of the second world war, after doctors in Germany were coerced and made complicit in crimes against humanity organized by the Third Reich. Freedom of conscience is something which is enshrined in the Canadian Charter of Rights and Freedoms and similar documents around the world.
For the vast majority of physicians practicing in Ontario, euthenasia is not something which they went into their job expecting to perform. When most were training at medical school, the understanding was that their job was simply to protect, preserve and save life as much as possible. For many of the senior physicians who graduated in the 1980s and 1990s, the idea of administering a medical death to patients and assisting in the dying process naturally goes against the grain of their very beliefs as a doctor.
Yet, when assisted dying was legalized by the federal government in 2016 and provinces were mandated with creating legislation around the issue, Ontario passed Bill 84, compelling all doctors to make an effective referral for medical assistant in dying and become implicated in the process.
The relatively threadbare legislation left many medical professionals groping in the dark, forced to create rules as they went along. One rule which it did impose was that of the aforementioned referral process.
Rather than simply putting patients in touch with the relevant services, an effective referral means that a doctor's name and details are attached to the referral, making the process more akin to a recommendation or even an endorsement.
“Our government is continuing to work with stakeholders in an effort to strike the right balance that supports patients, doctors and other health care professionals,” a spokesperson for the Ontario Minister of Health, Christine Elliott, told The Pointer. “This includes listening to Ontario doctors who have concerns with conscience protections.”
Under current law, euthanasia legislation requires regular review, so there will be a chance for Elliott and her ministry to visit the requests of doctors soon enough.

Ontario Minister of Health, Christine Elliott
The Ontario Health website outlines how the referral process works. “Doctors or nurse practitioners who are unable or unwilling to provide medical assistance in dying can also contact the care co-ordination service in order to refer their patients to doctors or nurse practitioners who can provide these services,” it says. “Pharmacists who are unable or unwilling to dispense medical assistance in dying drugs can also contact the care co-ordination service to make a referral.”
It must be acknowledged that there are two very passionate sides to this coin. Where many physicians feel uncomfortable being involved in the process of assisted suicide, many people are relieved and liberated by the fact they are allowed to legally end their life (and often suffering) with the help, support and comfort of the state. Indeed, many have no problem with the legislation in Canada and understand it to be hugely progressive.
Those who believe in the introduction of assisted dying are likely to oppose legislation increasing a physician’s power to conscientiously object. Since referrals are built into the core of healthcare in Ontario, fears could be raised about changes to mandatory referrals leading to restrictions and lower access to service. Though Gill suggests the opposite, any changes around allowing individual doctors to bring their religious or moral views into their professional duty to provide care could prejudice the system.
Gill told The Pointer that she’s not opposed to assisted suicide, but wants the power to “consciencously object” and not to take part. She wants an exemption, not a veto.
Gill makes her case on moral not religious grounds.
“Currently the biggest concern that doctors have is providing euthanasia, something which was considered to be homicide just three years ago,” Gill said. “For all the physicians practicing right now, this is something they never thought they’d be involved in; this isn’t what they went into medicine to do. When the legislation was coming forward, there was a survey done of Canadian physicians which found that nearly 70 percent of physicians did not feel comfortable providing MAiD or giving effective referrals for MAiD. Although the majority of physicians are happy with their patients having access to this, they do not want to be involved in the process.”
“Physicians have never been against providing patients with information,” she added “Physicians have always been more than happy to discuss all the options, they’re more than willing to provide patients with all the information they need to actually connect to the services they want. They’re more than willing to transfer the continuity of care. What they’re not willing to do is to provide effective referrals.”
More recent figures relating to physicians’ willingness to administer euthanasia are hard to come by. Few polls seem to have been gathered by impartial sources on the practice since it was made law in 2016. A selection of figures provided by the Canadian Medical Association in 2017 offer some insight into the issue, suggesting it is more complicated than the 70/30 split implied by Gill. According to the study, 62 percent of physicians in Canada would be willing to provide medical assistance in dying through an advance request, though 75 percent also say that they struggled with which circumstances met the criteria. Unsurprisingly, the situation is massively nuanced.
For Gill, the key detail is that of an effective referral and the role it plays. Some doctors, including many of religious persuasion in Brampton and Mississauga, are desperate to change that and step away from the process.
“Right now the way the Ontario model works is very flawed - it is forcing physicians to be a necessary intermediate step,” Gill explained. “It is actually blocking access because more than 1 million patients don’t have a family doctor… that actually acts as a barrier to care. If patients had open access, as they do in Alberta, they would have direct, barrier free access.”
With the chronic overcrowding in Ontario, it is perhaps unsurprising physicians are taking a major stand on this issue. Without freedom of conscience, Gill argues there is a risk of physicians becoming “robots” and losing the human element which is so vital in healthcare. The moral impact of administering a system some don’t believe in, combined with the harrowing and exhausting requirements of hallway healthcare, can be too much.

Overcrowding at Brampton Civic Hospital is an ongoing concern.
On the other hand, some would argue that the role of a physician is to provide assistance to patients with their requests. A doctor should listen to the patient and offer the best objective solution, which can involve operating without their own internal moral framework.
“The other part of this which is being missed - and is terrifying for doctors on the front line - we are seeing an escalating healthcare crisis,” Gill said. “We have seen billions of cuts and we have governments which are restricting and rationing access to frontline care, that’s why physicians are burning out. They’re burning out from moral injury.”
With her practice across the street from Brampton Civic Hospital, Gill says she sees first hand the extent of the hallway healthcare crisis.
“A patient of mine said that their husband had died in a Brampton [Civic] hallway because it was the only place for him to receive palliative care,” she said. “Since then we continue to have patients treated in appalling conditions. The doctors and nurses are trying to do their best, but we have the lowest amount of per capita funding for the entire province.”
This overcrowding and the availability of euthanasia services also provides an intense moral dilemma. Where assisted suicide services were first introduced to offer dignity in death to those who chose them, there is a danger that they offer a distopian solution to the costs of an aging population. Compounding this hypothesis, in Brampton Civic Hospital, the heart of the hallway healthcare crisis, adverts appear on waiting room monitors promoting the option of assisted suicide. With low funding for palliative care, Gill says it makes euthenasia seem like the only option, something she branded "appalling".
“We are baiting our most vulnerable patients, it costs approximately $50 to administer euthanasia, but a year's worth of palliative care can cost upwards of $20,000 per year. We have a growing and aging senior population, which is predicted to explode over the next few years, and governments don’t have a plan for it. They don’t have the funding or facilities to cope.”
For hospitals in Ontario - and growing cities like Brampton and Mississauga in particular - this sets a fairly ominous precedent. For some, the idea of no longer being able to function independently is terrifying. There are many who would choose to pass peacefully instead of struggling in palliative care for years - however, everyone should be offered the choice. The issue in Peel, with hospitals groaning under intense strain, is that many are offered the choice between substandard palliative care in a hospital hallway or a painless death.
Regardless of whether one considers euthanasia a moral issue or not, the choice should be there. To advertise assisted dying in hospitals, millions must be invested in improved palliative care for those who want it.
Between January 1 and October 31, 2018 there were 2,614 approved MAiD cases across the country, with more than 60 percent of cases relating to cancer.
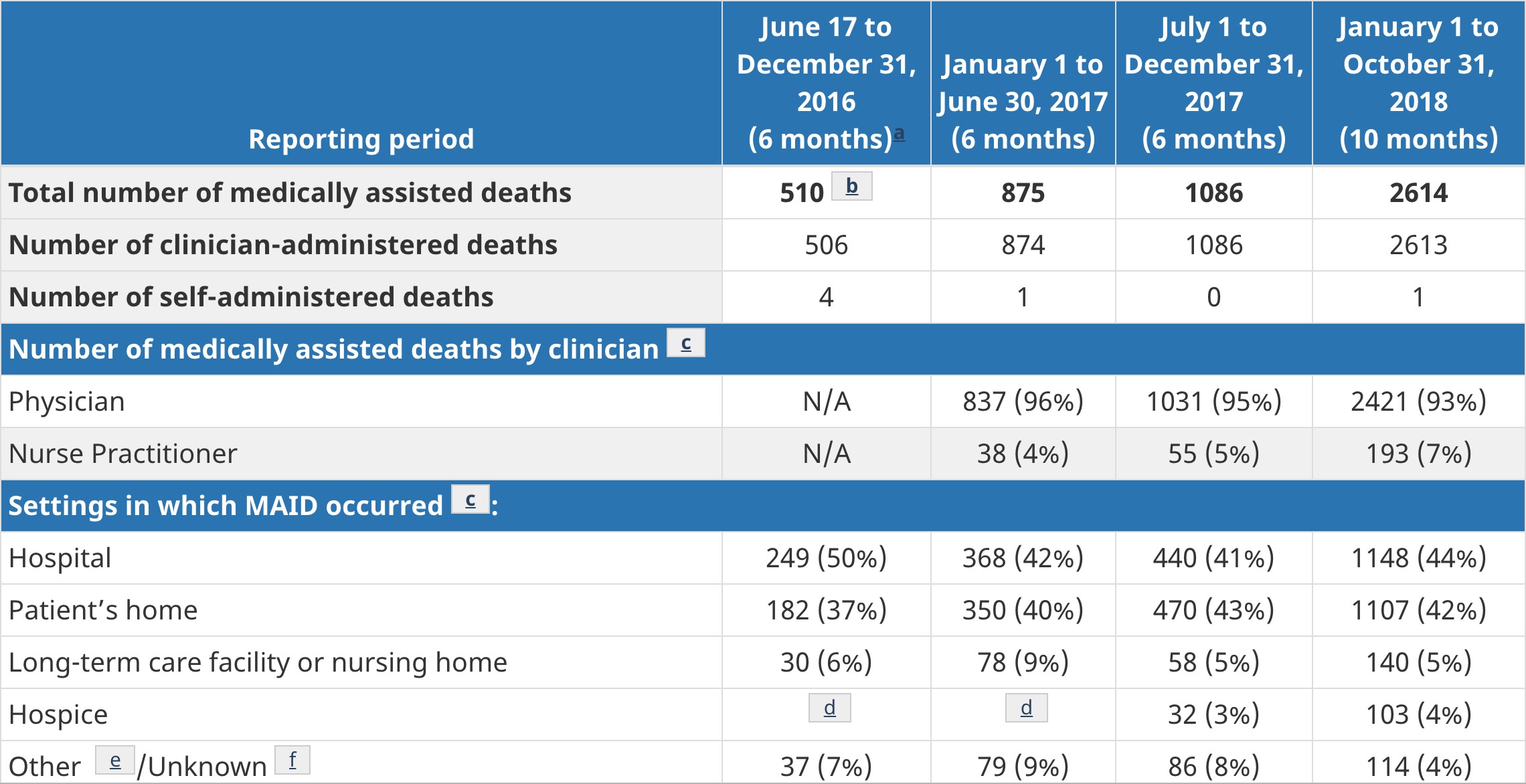
Statistics of medically assisted deaths and persons receiving MAID in Canada
(excludes: Quebec, Northwest Territories, Yukon, and Nunavut)
Doug Ford and the Progressive Conservatives recently rolled out their new healthcare initiative, launched in Mississauga, which heralded a new age of digital medicine. It suggested smart-policy such as video appointments to blend technological advancements into the heart of medicine. From an efficiency point of view, in a system where thousands are treated in hallways and closets, this new technological streamlined approach can bring benefits.
Some doctors, including Gill, worry that this technical efficiency in healthcare is being applied to them too. They see its rules around euthansia as a threat to their own morality and their ability to function within their own internal framework. Others, though, worry that even slight changes to the system, no matter how small, could threaten service provision and take away a right to assisted dying which many have fought hard for.
Email: [email protected]
Twitter: @isaaccallan
Tel: 647-651-4879
Submit a correction about this story
